��
ΰ��ĵ��̴���:Ϊʲô���͵��̴�����Ԥ�����ಡ
The Great Cholesterol Myth: Why Lowering Cholesterol Won��t Prevent Heart Disease and the Statin-Free Plan That Will
��
Jonny Bowden��ʿ
Jonny Bowden��ʿ��CNS��(��������åӪ��ѧ����)��һλȫ��֪���Ľ���ר�ҡ����Dz�ʿӵ��Ӫ��ѧ��ʿѧλ�����ڸ���ѵ�����˶���������6�������֤�����Ǽ�������������ߣ��������ڼ������ӽ�Ŀ�а���ר�ҵĽ�ɫ�����������Ozҽ���ķ�̸�У���������������ΰ��ĵ��̴��� The Great Cholesterol Myth�����������������վwww.jonnybowden.com�˽�������Jonny Bowden��ʿ����Ϣ��
��
��
���ಡ����Ҫԭ������֢��Inflammation)�� Ѫ�ܱڵ�С���˿��ɸ�Ѫѹ�Ͷ��أ��������ִ�л�����ϸ���������ͣ��Ѿ��ģ�LDL��������������ϵͳ�������������ϸ�����ӣ��������������֢���յ��°߿�����������յ������ಡ�ķ������ӡ����û����֢�������ͻᳩͨ��
��
��ͼͨ�����͵��̴���Ԥ�����ಡ����ͨ����������Ԥ������
������?��������ȥ��
ȥ�꣬���ಡѧ��Stephen Sinatra����һ��д��һ���顪����ΰ��ĵ��̴���:Ϊʲô���͵��̴�����Ԥ�����ಡ�Ͳ�Ҫ������ҩ��ƻ�ȴ����The Great Cholesterol Myth: Why Lowering Cholesterol Won��t Prevent Heart Disease and the Statin-Free Plan That Will�����������ţ�һ����ֵĻ�ϴ�����Ϣ����ѧ���п����ɵ��о�����ҵ��̰�����Լ���ƭ�Ե�Ӫ������ͬ������һ����ҽѧ��ʷ����ɴݻٺ��ƻ��Ե���:���̴��������ಡ��
��
��
�����ı������ڣ����ǰ�����ע�����������˵��̴��ϣ�ʵ���Ϻ��������ಡ��HEART DISEASE) ������ԭ��:��֢(INFLAMMATION)����������(OXIDATIVE DAMAGE)��ѹ��(STRESS)����(SUGAR)��ʵ���ϣ����ǿ���ͨ��ʳ�����������ʽ�ĸı�����һЩ���飬����Щ�ı������ҩ��ijɱ���Ҳû��ҩ��ĸ����á�
��
��
���ȣ������Ǵ�һЩ���˾��ȵ���ʵ��ʼ��
���̴������ಡ���Ǵ�Ҫ�ģ�
���̴�ˮƽ�����ಡ������һ���ܲ��Ԥ��ָ�ꣻ
һ������ಡ���������ڵ��̴������������ϣ�
���̴����ߵ�������һ�������ཡ����
���͵��̴����洦�������ޡ�
�Ҳ�û�����ó���Щ���ۣ���Ҳ�����������Щ���۵��档��ʮ���������̴���Ϊ���ಡ�IJ���(����������һ����Ҫ��־)һֱ���ȶ��ر���������ȡ�����Ϣ�Ǻ����ѵġ�(���ֶ����Ľ����̴�ҩ��Lipitor��Zocor��ÿ��Ϊ���ǵ������̴�����Լ340����Ԫ�����룬���ǶԱ��ֵ��̴����۵Ĵ������ǿ�ҵļȵ����档��������Ҳ����Ψһ���������ˡ��ҵ����Ѻ�Ӫ��ר��Terry Lemerond˵:��120�˷���������ҩ����ˣ�ֻ��һ�������档���������ϣ�ֻ�аٷ�֮һ���˻����档����ζ�ţ���100����ʹ�������ף�Lipitor����99������ÿ120��ʹ��Crestor�е�119�����ò����κκô���
�������Ը�⿼�Ǵ��Ƴ���˼άһ���ӣ�����������о�����ֻ���������������۵��ڶ�����֮һ��
�ﰺ��ʳ-�����о� (The Lyon Diet Heart Study)
��20����90����������о���Ա��������һ����Ϊ���ﰺ��ʳ-�����о���(Lyon Diet-Heart Study)��ʵ�飬�Բ��Բ�ͬ��ʳ�����ಡ��Ӱ�졣����ѡȡ�������ˣ����Ƕ��п��ܻ����ಡ��Σ�����ء����Ƕ���һ�����ಡ�������Ҵ������������иߵ��̴������̣����˶����кܸߵ�ѹ����һ������Ա��������������Э�����������ʳ��(�ͱ���֬���͵��̴�)����һ������Ը�������ĵ��к���ʳ��ŷ����-3֬���ᣬ�߲˺�����͵ȵ�һ������֬����
��
��
�����о���;ֹͣ�ˣ���Ϊ���к�������ಡ����������65%!!-�о���Ա��Ϊ������ȥ�Dz����µġ�
��
��
��
��ô����Ϊ��Щ�Ե��к���ʳ���˵ĵ��̴�ˮƽ��Σ������ʽ�����70% ? �����Ϊ����һ����ʯͷһ���������ˣ���?
�����롣���ǵĵ��̴�ˮƽ��û�иı䣬���о�ֹͣʱ�����ǵĵ��̴�ˮƽ���о���ʼʱһ���ߡ���Щ��ֻ��ֹͣ�����������̴��������ء�
������̴��������ಡ�IJ�������ʲô?
���ಡ����������
�����Ǽ�̵Ļش�: ���ಡ����Ҫԭ������֢��Inflammation)�� Ѫ�ܱڵ�С���˿��ɸ�Ѫѹ�Ͷ��أ��������ִ�л�����ϸ���������ͣ��Ѿ��ģ�LDL��������������ϵͳ�������������ϸ�����ӣ��������������֢���յ��°߿�����������յ������ಡ�ķ������ӡ����û����֢�������ͻᳩͨ��
��
��
��
��������Ϊ�������ಡ���յ��ߵ�ƻ��� ע�⣬���͵��̴����������档��Ҫע�����ѹ����
ѹ�������ಡ��һ������Ӧ�����ز�����֢��Ӧ������ܽ���Ϊʲô40%�Ķ�������Ӳ������û������Σ�����ء�����Terry��˵��������ϲ�������ּ���ѹ���ĸ����õIJݱ�ֲ���Ǻ쾰�� ��ӡ���˲Ρ������ܱȽ��͵��̴����õ�Ԥ�����ಡ��?
��
��
��
ע�����߸��ж���Ŀ������ܻᷢ�����������Ҫ���ĵ��̴���
1. �Կ�����ʳ��ˮ�����߲�������������Ȼ�Ŀ������ʣ�����Ƥ��(ƻ�������)�ͽ�����(������)�����̲��ʯ��֭��ƽ����ĵ����ʺ�֬���ʹ������߲ˡ��Ժ��ɿ��������ɿɻ��鴼�����ڽ���Ѫѹ��������Ѫ��ϵͳ�Ľ�����
2. ���ٹ�����ۡ��Ǻ�ŷ����-6֬����(ֲ����)��ÿһ�ֶ������Լ�����֢��
3. �������ѹ����ѹ�������ಡ��һ�����Σ�����أ�ͬʱҲ������֢���ҵ�һ�ַ��������������ӹ�ɢ������������ٵ���Ȫԡ���κ����鶼�а�����
4. �������������ǵ�������õĿ�˥��(�����ౣ��)ҩ�
5. �������ơ�����㲻�������ʶȡ�����ʣ��ǾͲ�Ҫ�Ⱦơ��ʶ���ָһ���һ�����ƣ�����������ĩ��7��14����
6. �����̡����������ಡԤ����ͷ�Ž��飻
7. ���ò�����������ࡰ����ӵ�С��IJ����: ����������ά����C����øQ10�� ŷ����-3֬���ᣬ���������ʺͽ����ء���Ȼ���Ƕ����м�ֵ����������ȴ��ͻ�����������Խ��Ƶ��������ȡ�����һ�ֿ��Ϳ���������������ֹ������תϸ�����ˡ��������յĽ�����ʵ���ϱȷ��������ҩ���粼��ҡ���ҩ�������������ơ�������̴���ǿ���ɣ�����Ч����û�и�����! ��ֻ�ǽ��������ô��е�һ�����ӡ���ʵ�ϣ���ӡ�ȣ����dzƽ�����Ϊ��һ�ֽ����������
��͡��ҩ���ƭ��
����һ���¡���������ҽ�������������͡��ҩ��ܾ���
��
��
Ҫ���µ�(����Ҫ��)���̴��������ԣ���ԶԶ���ڴ�ͳ�IJ��������������������������ĵ��̴�������������ĵ��ܶ�֬�������͡�(LDL-a�൱����;LDL-b����)���������һλŮ�ԣ���ע�⣬û��֤�ݱ�����͡��ҩ��������ȸ�Ů(���ͯ)����������֪�������о��У���͡��ҩ��ʹ�������ķ��ո��ߡ��������ˣ�Ҳ����59�����ϵ��ˣ����ߵĵ��̴�ʵ�������б������õġ�(������ҽ���Դ˱�ʾ���ɣ����Ƽ������������о�Framingham Study!)
��͡��ҩ��������DZ�ڵĸ����ã�����������ʹ������������ɥʧ���������˺�ƣ�͡����Ҫ֪��������͡��ҩ����˵��Ψһ�������ظ���Ψһ��Ⱥ���������ԣ�����ͨ��������40�굽59��֮�䣬������Ѫ�ܼ���(��ǰ�����ಡ����)�����ཡ��ר�һ��ɣ���ʹ�����ּ���С�ĺô���Ҳ������������͡��ҩ��Ŀ������ԣ����������ǽ��͵��̴���������
��
��
����
���͵��̴��ͽ��ͻ����ಡ�ķ�������ȫ��ͬ�ġ�
�����Ǻ���Ҫ�ġ�
ǰ�������ؽ�Ҫ�ġ�
_______________________________________________________________
��
��
The Great Cholesterol Myth: Why Lowering Cholesterol Won��t Prevent Heart Disease
By Dr. Jonny Bowden
Jonny Bowden, PhD, CNS, (aka "The Rogue Nutritionist™") is a nationally known health expert. Dr. Bowden has a PhD in nutrition, and has earned six national certifications in personal training and exercise. He is the author of several best-selling books, and appears regularly as an expert on several television programs, including a recent interview on the Dr. Oz show, discussing his book, The Great Cholesterol Myth. You can learn more about Dr. Jonny Bowden at his website, www.jonnybowden.com
Trying to prevent heart disease by lowering cholesterol is like trying to prevent obesity by cutting out lettuce.
Surprised? Read on.
Last year, cardiologist Stephen Sinatra and I came together to write a book��The Great Cholesterol Myth: Why Lowering Cholesterol Won��t Prevent Heart Disease and the Statin-Free Plan That Will. We believe that a weird admixture of misinformation, scientifically questionable studies, corporate greed, and deceptive marketing has conspired to create one of the most indestructible and damaging myths in medical history: that cholesterol causes heart disease.
The real tragedy is that by putting all our attention on cholesterol, we��ve virtually ignored the real causes of heart disease: inflammation, oxidative damage, stress and sugar. Things we can actually do something about by using food, supplements and lifestyle changes, none of which have the costs��nor the considerable side effects��of drugs.
First, let��s start with some surprising facts.
Cholesterol is a minor player in heart disease
Cholesterol levels are a poor predictor of heart attacks
Half of heart attacks happen to people with normal cholesterol
Half the people with elevated cholesterol have healthy hearts
Lowering cholesterol has an extremely limited benefit
I haven��t come to these conclusions lightly, and I wouldn��t expect you to take them at face value. The case against cholesterol as a cause of heart disease (or even as an important marker for it) has been crumbling steadily for decades, but getting the information out there is difficult. (The two top cholesterol lowering medications, Lipitor and Zocor, together bring in roughly 34 billion dollars a year for their makers, who have a strong vested interest in keeping the cholesterol theory alive. And they��re hardly the only ones who do.) My friend and fellow nutrition expert Terry Lemerond states that, ��Only one out of 120 people taking Crestor may benefit from the use of the drug. Only one out of 100 on Lipitor may benefit. That means 99 out of 100 taking Lipitor, and 119 out of 120 on Crestor would receive no benefits at all.��
But if you��re willing to consider breaking with conventional thinking for a minute, consider the following study, just one of the many we discuss in the book.
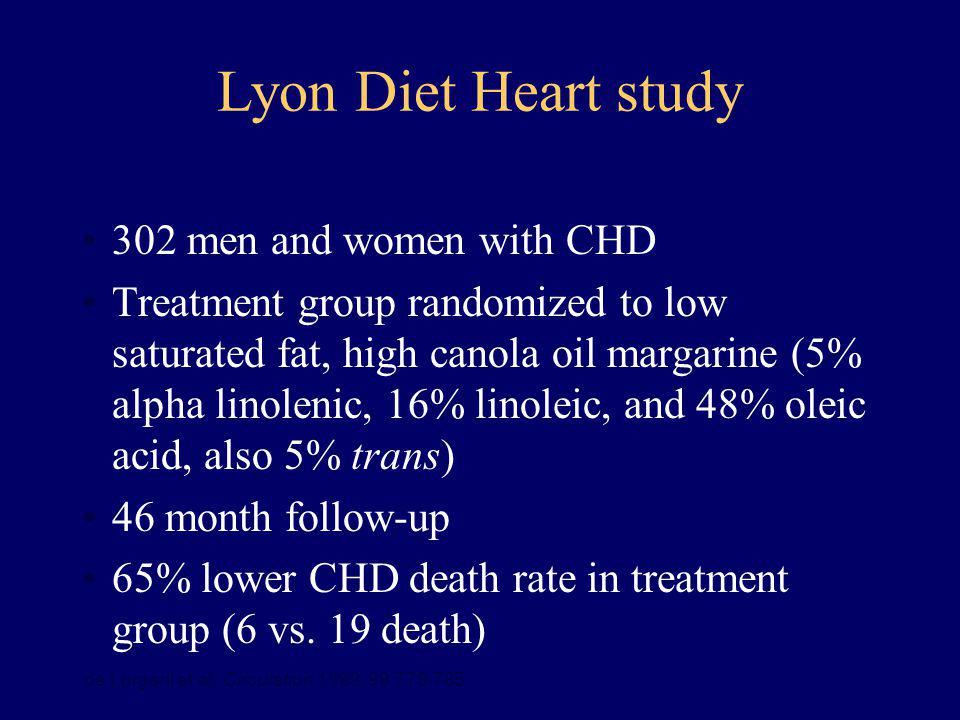
The Lyon Diet-Heart Study
In the 1990��s, French researchers decided to run an experiment- known as the Lyon Diet-Heart Study-- to test the effect of different diets on heart disease. They took two groups of men who had every risk factor for heart disease imaginable. All of them had survived a heart attack. They had high cholesterol, they smoked, they didn��t exercise and they had high levels of stress. Half the men were advised to eat the American Heart Association ��prudent diet�� (low saturated fat and cholesterol), while the other half were advised to eat a Mediterranean diet high in fish, omega-3s, vegetables and monounsaturated fat like olive oil.
The study was stopped midway because the reduction in heart attacks in the Mediterranean group was so pronounced��70%!!��that researchers decided it was unethical to continue.
So what do you think happened to the cholesterol levels in the men who ate the Mediterranean diet and had 70% reduction in deaths? You��d think they must have dropped like a rock, right?
Think again. Their cholesterol levels didn��t budge, and were just as high when the study was stopped as they were when the study began. The men just stopped dying. Cholesterol had nothing to do with it.
So if cholesterol isn��t the cause of heart disease, what is?
The Real Cause of Heart Disease
Here��s the short answer: The primary cause of heart disease is inflammation. Small injuries to the vascular wall that can be caused by anything from high blood pressure to toxins attract all sorts of metabolic riff-raff, from bacteria to oxidized (damaged) LDL particles; the immune system sends inflammatory cytokines to the area, and more oxidation and inflammation takes place eventually resulting in the growth of plaque and, ultimately, to an increased risk for heart disease. If there was no inflammation, the arteries would be clear.
Following is my seven point program for reducing the risk of heart disease. Note that lowering cholesterol isn��t on it. Note also that managing stress is.
Stress is a powerful contributor to heart disease. The stress hormones create inflammatory events that may explain why 40% of atherosclerotic patients have no other risk factors. According to Terry, his two favorite herbs for reducing the adverse effects of stress are rhodiola and ashwagandha. Could they be better for preventing heart disease than lowering cholesterol?
Pay attention to these seven action items, and you just may find that you don��t need to worry quite so much about cholesterol after all.
Eat an Anti-Inflammatory Diet. The fruit and vegetable kingdom is teeming with natural anti-inflammatories like quercetin (apples and onions) and curcumin (turmeric). Drink green tea and pomegranate juice. Balance your protein and fat with tons of vegetables. And eat dark chocolate��its cocoa flavanols help lower blood pressure and keep the cardiovascular system healthy.
Reduce grains, starches, sugar and omega-6s (vegetable oils). Every one of these has the power to increase inflammation��a lot!
Manage Your Stress. Stress is an enormous risk factor for heart disease, and is inflammatory as well. Find a way to manage it. Anything from regular walks in the park to deep breathing exercises to warm baths can help.
Exercise. It��s probably the best anti-aging (and heart protective) drug on the planet. In fact, if you are interested in an excellent daily regimen that yields great results, go to www.TerryTalksNutrition.com for the most efficient, time saving exercise program.
Drink only in moderation. And if you don��t process the word ��moderation�� very well, don��t drink at all. Moderation means one or two glasses of wine a day, not 7 to 14 glasses on the weekend!
Don��t smoke. Probably the number one recommendation for heart disease prevention.
Supplement smart. There are many ��must have�� supplements: antioxidants, vitamin C, coenzyme Q10, omega-3s, citrus bergamot, and curcumin. While they are all valuable, curcumin stands out. This amazing extract from turmeric does just about everything��it��s an anti-inflammatory and antioxidant, so it stops and even reverses cellular damage. However, it is vitally important to find a curcumin supplement that is clinically tested and absorbs well. My friend Terry Lemerond has found compelling evidence that a specific curcumin with up to 10 times the absorption of standard extracts is best on both of these counts. You take less, but get noticeably more benefits. This high-absorption curcumin is actually as effective as an anti-inflammatory than non-steroidal anti-inflammatory drugs like ibuprofen, celecoxib, naproxen sodium, and even the steroid, prednisone �C but without side effects! And that��s just one example of curcumin��s many achievements. In fact, in India, they call curcumin ��the all in one solution.��
The Statin Scam
And one more thing��if your doctor wants to put you on a statin drug, push back!
Ask for the newer (and far more important) cholesterol particle tests, which go well beyond old-fashioned measurements like ��good�� and ��bad�� cholesterol and actually tell you what type of LDL you have. (LDL-a is pretty harmless; LDL-b is not.) If you��re a woman, be aware that there��s no evidence that statin drugs save lives in women (or children!). Know that in a number of studies, statin users have a higher risk for diabetes. And that in older people, meaning over 59 years of age, higher cholesterol is actually protective. (If your doctor doubts that, refer him to the Framingham Study!)
Statin drugs have many potential side effects, including muscle pain and weakness, memory loss, diminished libido and fatigue. Finally, know that the only population for which a modest��repeat, modest��benefit for statin drugs has been consistently shown is middle aged men generally between the age of 40 and 59 with existing cardiovascular disease (previous heart attack). And many health professionals suspect that even this extremely modest benefit is probably due to the anti-inflammatory nature of statins, rather than their ability to lower cholesterol.
The Bottom Line
Lowering cholesterol and lowering the risk of heart disease are very far from the same thing.
The latter is important.
The former is almost irrelevant.
_______________________________________________________________
Jonny Bowden, PhD, CNS, aka ��the Rogue Nutritionist™�� is a board-certified nutritionist and the co-author (with cardiologist Stephen Sinatra, MD) of ��The Great Cholesterol Myth: Why Lowering Cholesterol Won��t Prevent Heart Disease and the Statin-Free Plan That Will�� (Fairwinds, 2012)
https://www.terrytalksnutrition.com/health-articles/the-great-cholesterol-myth/
��
Ann Transl Med. 2019 Apr; 7(7): 147.
Anti-inflammatory therapy for cardiovascular disease
Constantine E. Kosmas,corresponding author1 Delia Silverio,2 Andreas Sourlas,3 Peter D. Montan,2 Eliscer Guzman,1 and Mario J. Garcia1
Author information Article notes Copyright and License information Disclaimer
1Department of Medicine, Montefiore Medical Center, Bronx, NY, USA;
2Cardiology Clinic, Cardiology Unlimited, PC, New York, NY, USA;
3School of Medicine, University of Crete, Heraklion, GreecAbstract
Chronic subclinical inflammation is a central process in the pathogenesis of cardiovascular disease (CVD) and it has been linked with both the initiation and progression of atherosclerosis. Several pro-inflammatory cytokines, such as the C-reactive protein (CRP), tumor necrosis factor-�� (TNF-��) and interleukin-6 (IL-6) have been described as independent risk factors for coronary heart disease and promoters of atherogenesis. Thus, extensive research is being conducted to assess the role of anti-inflammatory therapy in the primary and secondary prevention of CVD. Our review aims to provide the clinical and scientific data pertaining to the effects of different anti-inflammatory agents administered in patients with CVD.
Keywords: Inflammation, pro-inflammatory cytokines, anti-inflammatory agents/therapy, cardiovascular disease (CVD)Hydroxychloroquine (HCQ)
HCQ, a disease-modifying antirheumatic drug (DMARD), is an immunosuppressant agent used in the management of certain autoimmune diseases, such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), as well for the prevention and treatment of certain types of malaria (18).
It exerts its immunomodulatory properties by suppressing inflammatory pathways through the prevention of toll-like receptor activation, which is needed for the expression of interferon-regulated genes and for the production of TNF-��, a major component of the cell-mediated inflammatory response (18,19).
High-dose HCQ therapy (400 mg daily), has been independently associated with a 56.8% reduced risk for CV morbidity in patients with RA (20).
In a retrospective study, which included 1,266 patients with incident RA (excluding patients with CVD prior to RA diagnosis), HCQ use was associated with a 72% reduction in the risk of incident CVD and a 70% reduction in the risk of the composite incident CAD, stroke, and transient ischemic attack (TIA) (21).
Furthermore, there is evidence that HCQ exhibits hypolipidemic, hypoglycemic and antithrombotic properties when administered in patients with autoimmune diseases, such as RA or SLE (19,22-24), which may significantly contribute in the reduction of the risk for CVD conferred by HCQ in these patients.
Phospholipase A2 (PLA2) inhibitors
PLA2 is a widely distributed group of enzymes found in many isoforms, including the lipoprotein-associated phospholipase A2 (Lp-PLA2), cytosolic phospholipase A2 (cPLA2) and secretory phospholipase A2 (sPLA2) (42).
PLA2 enzymes hydrolyze phospholipids to generate free fatty acids and lysolipids, which are key components for the biosynthesis of eicosanoids and platelet-activating factor (PAF), thus potently promoting inflammation and atherogenesis (43,44). Both, Lp-PLA2 and sPLA2 are expressed primarily in pro-atherogenic inflammatory cells including macrophages, monocytes and lymphocytes (42,44). Furthermore, several sPLA2 are expressed with various patterns in all stages of atherosclerosis development (44,45).
In addition, both Lp-PLA2 and sPLA2, to a different extent, are carried by LDL and generate lysophosphatidylcholine (Lyso-PC) and oxidized fatty acid (oxFA), two pro-inflammatory mediators promoting cell activation and production of inflammatory cytokines. Furthermore, Lyso-PC may also perpetuate vascular inflammation and promote necrotic core formation in atheromatous plaques, thus making plaques susceptible to rupture (46).
Given the above described pro-inflammatory and pro-atherogenic properties of PLA2 enzymes, it becomes well understandable why PLA2 inhibitors have received considerable attention in the medical research field as drug targets for the prevention and management of CVD. Two PLA2 inhibitors have been developed, varespladib and darapladib.Anti-inflammatory therapy for cardiovascular disease
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6511577/��
��
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
