��
Methemoglobinemia is main clinical conditions of sodium nitrite intoxification.
Dozens of drugs that have oxidizing effects can cause methemoglobinemia.
Methylene blue is the first line treatment, but with risks to worsen the condition.
Vitamin C is an effective treatment.
Vitamin is a strong reducing agent, can convert ferric iron back to ferrous state.
Glucose, also as a reducing agent, is helpful.
vitamin c is the outstanding antioxidant in the plasma. UC Berkely, 1989
��
��
Methemoglobinemia����Ѫ����Ѫ֢ is a hemoglobinopathy caused by high levels of methemoglobin that result from oxidation of ferrrous (Fe2+) to the ferric state (Fe3+) in hemoglogin. Methemoglobin cannot carry oxygen, leading to tissue hypoxia.
Anesthetic experience of methemoglobinemia detected during general anesthesia for gastrectomy of advanced gastric cancer -A case report-
We present a 68-year-old female patient who underwent gastrectomy for advanced gastric cancer with bleeding.
...
Ascorbic acid 600 mg mixed in fluid was administered, and methylene blue 1 mg/kg was intravenously injected slowly over 3 minutes. The methemoglobin level reduced to 11.2% after the administration of ascorbic acid and reduced to 4.3% and then 2.3% after methylene administration.
Dapsone is a sulfone antibiotic used for the treatment of Hansen's disease and other dermatologic diseases, as well as in immunosuppressed patients to prevent pneumocystitis carinii pneumonia or organ transplant patients, especially those intolerant to sulfonamide. Methemoglobinemia is a known side-effect of dapsone [4-6] and the patients of most cases had a history of dapsone-intake. The patient here had a 30-year history of dapsone-intake, although this information was not obtained initially. Dapsone is almost completely absorbed in the gastrointestinal track and passes the enterohepatic circulation. Only 20% of the dosage-intake is excreted into the urine. The plasma half-life varies from 10 to 80 hours and is dose-dependent.
Anesthetic experience of methemoglobinemia detected during general anesthesia for gastrectomy of advanced gastric cancer -A case report-
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2998655/��
��
Vitamin C: Why we need it, dietary sources, and how we absorb and metabolize it - YouTube
https://www.youtube.com/watch?v=vcLzhCPuAmw��
��
��
American Journal of Therapeutics: July/August 2014
Ascorbic Acid for the Treatment of Methemoglobinemia: The Experience of a Large Tertiary Care Pediatric Hospital
Rino, Pedro Bonifacio MD; Scolnik, Dennis MBChB; Fustiñana, Ana MD; Mitelpunkt, Alexis MD; Glatstein, Miguel MDAuthor Information
1Division of Pediatric Emergency Medicine, Hospital de Pediatr��a Prof. Dr. Juan P. Garrahan, Buenos Aires, Argentina;
2Division of Pediatric Emergency Medicine, Department of Pediatrics, The Hospital for Sick Children, University of Toronto, Ontario, Canada;
3Division of Clinical Pharmacology and Toxicology, The Hospital for Sick Children, University of Toronto, Ontario, Canada;
4Division of Pediatric Emergency Medicine, Department of Pediatrics, Dana-Dwek Children Hospital, University of Tel Aviv, Tel Aviv, Israel; and
5Division of Clinical Pharmacology and Toxicology, Ichilov Hospital, University of Tel Aviv, Tel Aviv, Israel.
The purpose of reporting this series of patients is to illustrate the role of ascorbic acid in the treatment of severe acquired methemoglobinemia (metHb), especially when methylene blue is not available. Medical records of affected patients were reviewed to collect history of exposures, food ingestion, physical examination, pulse oximetry, blood gas, and co-oximetry results, and outcomes. Five cases of acquired metHb are presented here, all of whom received treatment with ascorbic acid and fully recovered after 24 hours of treatment. Our series emphasizes that ascorbic acid is an effective alternative in the management of acquired metHb if methylene blue is unavailable and suggests that ascorbic acid infusion may be indicated in patients with glucose-6-phosphatase dehydrogenase deficiency.����Ѫ�����Ƹ���Ѫ����Ѫ֢:һ����������ҽԺ�ľ���
Pedro Bonifacioҽѧ��ʿ;����˹MBChB Scolnik;Fustinana,����ҽѧ��ʿ;Mitelpunkt Alexisҽѧ��ʿ;Miguel MDAuthor��Ϣ
1����͢����ŵ˹����˹ʥĸҽԺ���Ƽ��ﲿJuan P. Garrahan����;
2���ô���ʡ�����ѧ����ҽԺ���ƶ��Ƽ���ҽѧ��;
3���ô���ʡ�����ѧ����ҽԺ�ٴ�ҩ��ѧ�Ͷ���ѧ��;
��ɫ������ά���ѧ����-��³�˶�ͯҽԺ���Ƽ����;��
��ɫ������ά���ѧ�������ҽԺ�ٴ�ҩ��ѧ�Ͷ���ѧ�ơ�
������һϵ�л��ߵ�Ŀ����Ϊ��˵������Ѫ�����������ػ���Ը����쵰��Ѫ֢(metHb)�е����ã��ر��ǵ�û���Ǽ���ʱ���ع���Ӱ�컼�ߵ�ҽ�Ƽ�¼���ռ���¶ʷ��ʳ����ʳʷ�������ʷ������Ѫ������ʷ��Ѫ������Ѫ����������ͽ�������ı���5������Լ��������λ��ߣ������ܿ���Ѫ�����ƣ�24Сʱ����ȫ���������ǵ�ϵ��ǿ�������û���Ǽ���������Ѫ�������ƻ���Ը����쵰��Ѫ֢(metHb)����Ч���Ʒ�������飬����Ѫ����ע������������-6����ø����øȱ��֢���ߡ�Ascorbic Acid for the Treatment of Methemoglobinemia: The E... : American Journal of Therapeutics
https://journals.lww.com/americantherapeutics/Abstract/2014/07000/Ascorbic_Acid_for_the_Treatment_of.3.aspx��
����Ѫ��������������ʽ���ε��ŵ�
Advantages of Ferrous Ascorbate on other forms of iron salts
2016.8.21 GUPTA����0����
������֯�����Ϲ���ͯ����Ὠ�飬��40%��ƶѪ֢���й��ҵ�������������ÿڷ����������������ڷ����䷽��������������ʽ�ṩ��Ҳ���ɶ���ѿ������������ɵ������������ʽ�ṩ����Щ���������ڰ�ȫ�ԡ�������Ч�ԡ��ɱ������÷�����ڲ��졣�������г��Ͽɻ�õIJ�ͬ��ѧ״̬�����䷽������Ҳ�����ڲ�ͬ��galenic��ʽ��
�ٴ��ϣ������������������������������������ȶ������ε�Ӧ�ñ����θ�Ϊ�㷺��������ʽ�������������öȱȺ�����ʽ�ĵ�3 - 4��(�������ö�Ϊ10 - 15%)�����������ڼ�����Һ�����ܣ�����ڱ�����֮ǰ����ת��Ϊ����������
�ڷ����Ƽ���ѭ��ͳ�ġ��ӳ��ͷš��䷽�������θ����������������������������öȡ���������ʽ���պ�����ѪҺ�дﵽ���ֵԼ7Сʱ��������24Сʱ��
����Ѫ�������ǿ���Ѫ��������Ӧ�IJ���ڿ���Ѫ����ڵ�����£������ܺõ����գ���Ϊ���ֻ����ﱻ��Ϊ�ܰ���ת��Ϊ�����������͵���������pHֵ�¿��ܣ��ɱ����������͵������ա�����Ѫ����Է�ֹ�����������������Ϊ��ԭ�������������ĺ�ɫ��ʽ���������뿹��Ѫ����ȶ����ϣ�����Ѫ����������Ϊ�������ش�����θ�����ڡ����ֻ����ﲻ�������κ�ʳ�����Ƽ������롣���ڿ���Ѫ�������������������������о����֣�����Ѫ��������ˮ��Һ�н���Ϊ����Ѫ�����Ӻ��������ӣ����п���Ѫ�������Ե�����ʽ���ڡ�����Ѫ����֪��pH5���롣��pH6 ~ 8ʱ������Ѫ����ǿ���ܽ�ȣ������ڿ���Ѫ�����������ա�
��18������־Ը�߽������ٴ��о����Ƚ��˿���Ѫ���������������䷽��21�����������������졣���ǣ������Ѫ�쵰�������ﵽ�˻���ֵ�����о�С�黹��������һ���о�����������(FeIII�����������ѿ��)���������ö��������(����Ѫ������)���������öȽ����˱Ƚϡ�ͨ������Ѫ�����������ߺ�ȫ��������ֵ�������ո�״̬�³����е������ա�Ѫ������FeIII����(1.2+/- 0.1%)���ڿ���Ѫ����43.7+/- 7.1%����ʳ�����������ձ仯���������������ձ仯��
�ڿ���100mg��28��Ĵ��������䷽��Ѫ�쵰��ˮƽ�������䷽�ĸߡ�����һЩ���Ƶ��о��Ѿ�֤����������ʽ������Ѫ��������������ʽ�������и�����������öȡ���ˣ����Ʊ�ҩ��ʱ���������ر��ǿ���Ѫ�������α���������ʽ����Ч���ɱ�Ч��ߣ������Ժá�Advantages of Ferrous Ascorbate on other forms of iron salts | PHARMA FRANCHISE
http://pharmaceuticalcompanyindia.in/advantages-of-ferrous-ascorbate-on-other-forms-of-iron-salts/��
��
Clin Exp Emerg Med. 2018 Sep; 5(3): 192�C198.
Therapeutic effect of ascorbic acid on dapsone-induced methemoglobinemia in rats
Changwoo Kang,1,2 Dong Hoon Kim,1,2 Taeyun Kim,1 Soo Hoon Lee,1,2 Jin Hee Jeong,1 Sang Bong Lee,1 Jin Hyun Kim,2,3 Myeong Hee Jung,3 Kyung-woo Lee,4 and In Sung Park2,5
Abstract
Objective
Dapsone (diaminodiphenyl sulfone, DDS) is currently used to treat leprosy, malaria, dermatitis herpetiformis, and other diseases. It is also used to treat pneumocystis pneumonia and Toxoplasma gondii infection in HIV-positive patients. The most common adverse effect of DDS is methemoglobinemia from oxidative stress. Ascorbic acid is an antioxidant and reducing agent that scavenges the free radicals produced by oxidative stress. The present study aimed to investigate the effect of ascorbic acid in the treatment of DDS induced methemoglobinemia.
Methods
Male Sprague-Dawley rats were divided into three groups: an ascorbic acid group, a methylene blue (MB) group, and a control group. After DDS (40 mg/kg) treatment via oral gavage, ascorbic acid (15 mg/kg), MB (1 mg/kg), or normal saline were administered via tail vein injection. Depending on the duration of the DDS treatment, blood methemoglobin levels, as well as the nitric oxide levels and catalase activity, were measured at 60, 120, or 180 minutes after DDS administration.
Results
Methemoglobin concentrations in the ascorbic acid and MB groups were significantly lower compared to those in the control group across multiple time points. The plasma nitric oxide levels and catalase activity were not different among the groups or time points.
Conclusion
Intravenous ascorbic acid administration is effective in treating DDS-induced methemoglobinemia in a murine model.In this study, we demonstrated that intravenous ascorbic acid administration was effective at reducing methemoglobin levels. However, ascorbic acid was slightly less effective than methylene blue administration. At 120 minutes, the methemoglobin concentration of the ascorbic acid group was not significantly different from that of the control group, whereas the methylene blue group showed a more marked difference. In actual clinical cases, because the therapeutic response to ascorbic acid is less marked, repeated doses of intravenous ascorbic acid or an oral preparation have been prescribed, whereas we administered a single intravenous dose of ascorbic acid [20,26]. Furthermore, we administered 15 mg/kg of ascorbic acid in doses determined in a pilot study. Therefore, a higher dose of ascorbic acid might be needed to achieve better therapeutic results.
Keywords: Methemoglobin, Ascorbic acid, Methylene blue, Anti-oxidationTherapeutic effect of ascorbic acid on dapsone-induced methemoglobinemia in rats
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6166037/��
Effective role of ascorbic acid as an alternative treatment of methemoglobinemia: A case report
Introduction: Methemoglobinemia is a rare
clinical disorder characterized by increase in the
blood level of methemoglobin (MetHb) which
leads to tissue hypoxia. Methemoglobinemia
may be congenital, but acquired type is more
common and occurs after exposure to oxidizing
agents. Treatment of choice is methylene blue
(MB). The side effects of MB restrict its usage
in special conditions. Ascorbic acid is a good
alternative drug with limited experience in
methemoglobinemia. Case Report: Eight years
old male patient presented with cyanosis
after dapsone exposure and diagnosis of
methemoglobinemia was confirmed. The
patient was managed successfully with
ascorbic acid. Conclusion: Ascorbic acid
could be used as an alternative treatment for
methemoglobinemia when methylene blue is
not available or contraindicated.
Keywords: Ascorbic acid, Dapsone, Methemoglobinemia
INTRODUCTION
Methemoglobinemia is a medical emergency requiring
immediate treatment. Methemoglobinemia is a condition
in which iron atom in hemoglobin is transformed form
a ferrous (Fe2+) state to a ferric (Fe3+) state due to effect
of oxidizing agent exposure. Thus, beside the inability
of methemoglobin (MetHb) to carry O2
, MetHb shifts
the oxygen - hemoglobin dissociation curve to the left,
hindering the release of O2
to the tissues [1]. There
are many drugs and toxins such as nitrate, dapsone,
prilocaine, antimalarial drugs and sulphonamides
responsible for acquired methemoglobinemia [2].
Methylene blue (MB) is considered the commonest and
the usual treatment of methemoglobinemia which may
lead to serious complications and also it is contraindicated
in some patients like those with glucose-6-phosphate
dehydrogenase (G6PD) deficiency [3]. In this case report,
we presented a child with methemoglobinemia induced
by dapsone and the patient was treated and improved
with ascorbic acid to highlight its effectiveness as an
alternative treatment.
After confirming diagnosis, dapsone was stopped
and the child was kept on oxygen inhalation by nasal
prong, while on oxygen, the saturation only raised to
83%.Multiple dose activated charcoal 1g/kg was given
orally to the child, methylene blue was not available,
thus slow intravenous administration of 1gm ascorbic
acid was started . Injection ascorbic acid was continued
as 1gm/4hs (for 8 doses), no side effects occurred. The
child showed signs of improvement, saturation gap and
cyanosis disappeared, MetHb level was repeated after six
hours of ascorbic acid therapy, day two and day three of
admission which was 12.6%, 5.7% and 1.9% respectively,
indicating successful therapy with ascorbic acid. The
child was discharged with full recovery on the third day
of admission.
Dapsone induces a continuing oxidative stress
due to the long half-life, thus serial measurements
of methemoglobin levels should be done [4]. Initial
management of acquired methemoglobinemia inculdes
identification and discontinuation of the offending agent
and increasing tissue oxygenation by administration of
reducing agent as MB and ascorbic acid [1].
Methylene blue is the usual treatment for
methemoglobinemia, however methylene blue is
potentially hazardous. Methylene blue can conversely
cause methemoglobinemia in high doses by its oxidant
effect and induce hemolysis in cases of G6PD deficiency in
addition to turning the skin blue, which is the commonest
side effect [2, 7]. Therefore, alternative treatments are
required. Ascorbic acid is a strong reducing agent that
takes part in many oxidation�Creduction reactions,
so ascorbic acid directly reduce methemoglobin and
is proven to treat cyanosis [3]. In many case reports,
ascorbic acid was used successfully in treatment of
methemoglobinemia with different doses and durations
as discussed in Table 2 [8�C10]. In the present case, a
decline of 12.2% in methemoglobin levels after six hours
of administration of 2 g ascorbic acid was noticed.
On contrary, other study reported that acquired
methemoglobinemia does not respond to ascorbic
acid, because its capacity to reduce MetHb is much
inferior to that of endogenous enzymatic systems
[11]. However, failure of ascorbic acid in treatment of
methemoglobinemia could be attributed to using lower
doses or shorter durations of therapy [2].100077Z01EM.pdf
http://www.ijcasereportsandimages.com/archive/2018-pdfs/2018100077Z01EM-mohammed/100077Z01EM.pdf��
stion, physical examination, pulse oximetry, blood gas, and co-oximetry results, and outcomes. Five cases of acquired metHb are presented here, all of whom received treatment with ascorbic acid and fully recovered after 24 hours of treatment. Our series emphasizes that ascorbic acid is an effective alternative in the management of acquired metHb if methylene blue is unavailable and suggests ...
Effective role of ascorbic acid as an alternative treatment of ��
www.ijcasereportsandimages.com/archive/2018-pdfs/2018100077Z01EM... �� PDF �ļ�ascorbic acid. Conclusion: Ascorbic acid could be used as an alternative treatment for methemoglobinemia when methylene blue is not available or contraindicated. Keywords: Ascorbic acid, Dapsone, Methemo-globinemia Eman Abdelfath Mohammed 12 1
��
Toxicology and Applied Pharmacology
Volume 21, Issue 2, February 1972, Pages 176-185
Toxicology and Applied Pharmacology
Ascorbic acid and chemically induced methemoglobinemias��
John Z.BolyaiabRoger P.Smithab2Clarke T.Grayab
a
Department of Pharmacology and Toxicology, Dartmouth Medical School, Hanover, New Hampshire 03755 USA
b
Department of Microbiology, Dartmouth Medical School, Hanover, New Hampshire 03755 USA
Received 18 March 1971, Available online 24 September 2004.
Abstract
Sodium nitrite was added to suspensions of washed guinea pig red cells in concentrations which converted about a third of the total blood pigment to methemoglobin. Various aliquots also contained added ascorbic acid in concentrations of 0.05, 0.5, or 5.0 mm (��physiological�� levels are between 0.05 and 0.1 mm). Methemoglobin levels were followed for 2 hr at 37��C. None of the tested concentrations of ascorbate significantly attenuated methemoglobin formation. On the contrary, significantly higher methemoglobin levels were sometimes found with 5.0 mm ascorbate. Guinea pigs were maintained several weeks on a scorbutogenic diet with or without ascorbate supplementation in their water. When blood ascorbate levels were significantly different, both groups were given intraarterial sodium nitrite, 40 mg/kg, and methemoglobin levels were followed with time as above. At none of the sampling times was there a significant difference in the methemoglobin levels between the 2 groups. As judged by the appearance of radioactivity in blood at various times after sc injection, the two groups also showed no difference in the rates at which they absorbed KS14CN. In human red cell suspensions 5.0 mm ascorbate significantly attenuated the methemoglobinemic response to tested concentrations of sodium nitrite, hydroxylamine and phenylhydroxylamine at 1 hr, but lower concentrations of ascorbate were without effect. When human red cells were first exposed to nitrite, then washed and ascorbate added, significant acceleration of methemoglobin reduction was observed with 5.0 mm ascorbate at 12, 24, and 36 hr, and with 0.5 mm ascorbate at 12 and 24 hr. In contrast, the oxygen capacities of suspensions with 5.0 mm ascorbate were significantly higher than control only at 12 and 24 hr, whereas with 0.5 mm ascorbate they were significantly higher at 12, 24, and 36 hr. In plain buffer, 5.0 mm ascorbate produced a small but significant loss of the tested concentration of sodium nitrite within 2 hr, but not at shorter intervals or at lower ascorbate concentrations.Ascorbic acid and chemically induced methemoglobinemias - ScienceDirect
https://www.sciencedirect.com/science/article/pii/0041008X72900609��
WHAT TREATMENT WORKS?
The course of hereditary methemoglobinemia type I is benign, but these patients should not be administered oxidant drugs. Treatment may be required for cosmetic reasons or for an inadvertent use of oxidant drugs. Ascorbic acid, 300 to 600 mg orally daily divided into 3 or 4 doses, is helpful.15
For methemoglobinemia due to drug exposure, traditional first-line therapy consists of an infusion of methylene blue, whose action depends on the availability of reduced nicotinamide adenine nucleotide phosphate (NADPH) within the red blood cells. After an acute exposure to an oxidizing agent, treatment should be considered when the methemoglobin is 30% in an asymptomatic patient and 20% in a symptomatic patient.16 Patients with anemia or cardiorespiratory problems should be treated at lower levels of methemoglobin. Methemoglobinemia due to hemoglobin M does not respond to ascorbic acid or methylene blue.
Dextrose should be given17 because the major source of NADH in the red blood cells is the catabolism of sugar through glycolysis. Dextrose is also necessary to form NADPH through the hexose monophosphate shunt, which is necessary for methylene blue to be effective.
Methylene blue is an oxidant; its metabolic product leukomethylene blue is the reducing agent. Therefore, large doses of methylene blue may result in higher levels of methylene blue rather than the leukomethylene blue, which will result in hemolysis and, paradoxically, methemoglobinemia in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency.18 Patients with G6PD deficiency also may not produce sufficient NADPH to reduce methylene blue to leukomethylene blue; thus, methylene blue therapy may be ineffective in these patients.18
Some drugs, such as dapsone, benzocaine, and aniline, produce a rebound methemoglobinemia, in which methemoglobin levels increase 4 to 12 hours after successful methylene blue therapy.19
N-Acetylcysteine, cimetidine, and ketoconazole are experimental therapies in the treatment of methemoglobinemia that have shown some promising results.20,21,22 Exchange transfusion is reserved for patients in whom methylene blue therapy is ineffective.Drugs or toxins that can cause methemoglobinemia*
Acetanilid
Alloxan
Aniline
Arsine
Benzene derivatives
Benzocaine
Bivalent copper
Bismuth subnitrate
Bupivacaine hydrochloride
Chlorates
Chloroquine
Chromates
Clofazimine
Dapsone
Dimethyl sulfoxide
Dinitrophenol
Exhaust fumes
Ferricyanide
Flutamide
Hydroxylamine
Lidocaine hydrochloride
Metoclopramide hydrochloride
Methylene blue
Naphthalene
Nitrates
Nitric oxide
Nitrites
Nitrofuran
Nitroglycerin
Sodium nitroprusside
Paraquat
Phenacetin
Phenazopyridine hydrochloride
Phenol
Phenytoin
Prilocaine hydrochloride
Primaquine phosphate
Rifampin
Silver nitrate
Sodium valproate
Smoke inhalation
Sulfasalazine
Sulfonamides
TrinitrotolueneEvidence-Based Case Review: Methemoglobinemia
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1071541/��
Sodium Nitrite
(Redirected from SN)
��All-meat regimen cured my depression.��
�D Jordan Bernt Peterson, Canadian psychologist and professor of psychology
Sodium nitrite (SN), mainly used in preserving processed meats and fish, has been mentioned in murder cases, suicide cases, and accidental poisoning cases. A list of such incidents in medical literature has been documented in Sodium Nitrite Poisoning Cases, as well as anecdotal experiences from forum users[Archive].
Contents
1 Simple step-by-step instructions
2 How it works
3 Sodium nitrite
4 Antiemetics
5 Antacids
6 Required time
7 Consequences of failure
8 Success stories on the news
9 Tips
10 Where to find
11 Further Reading
12 References
Simple step-by-step instructions
There are many ways to commit suicide by sodium nitrite. The following is an easy, quick, and pain-free recipe.
1. Take 30 mg metoclopramide (another editor suggested 800 mg of Tagamet, as well).
2. Wait 1 hour.
3. Dissolve 15 �C 25 g sodium nitrite in 50 �C 100 ml water.
4. Drink the solution and relax on a bed, a couch, or a reclining chair.
How it works
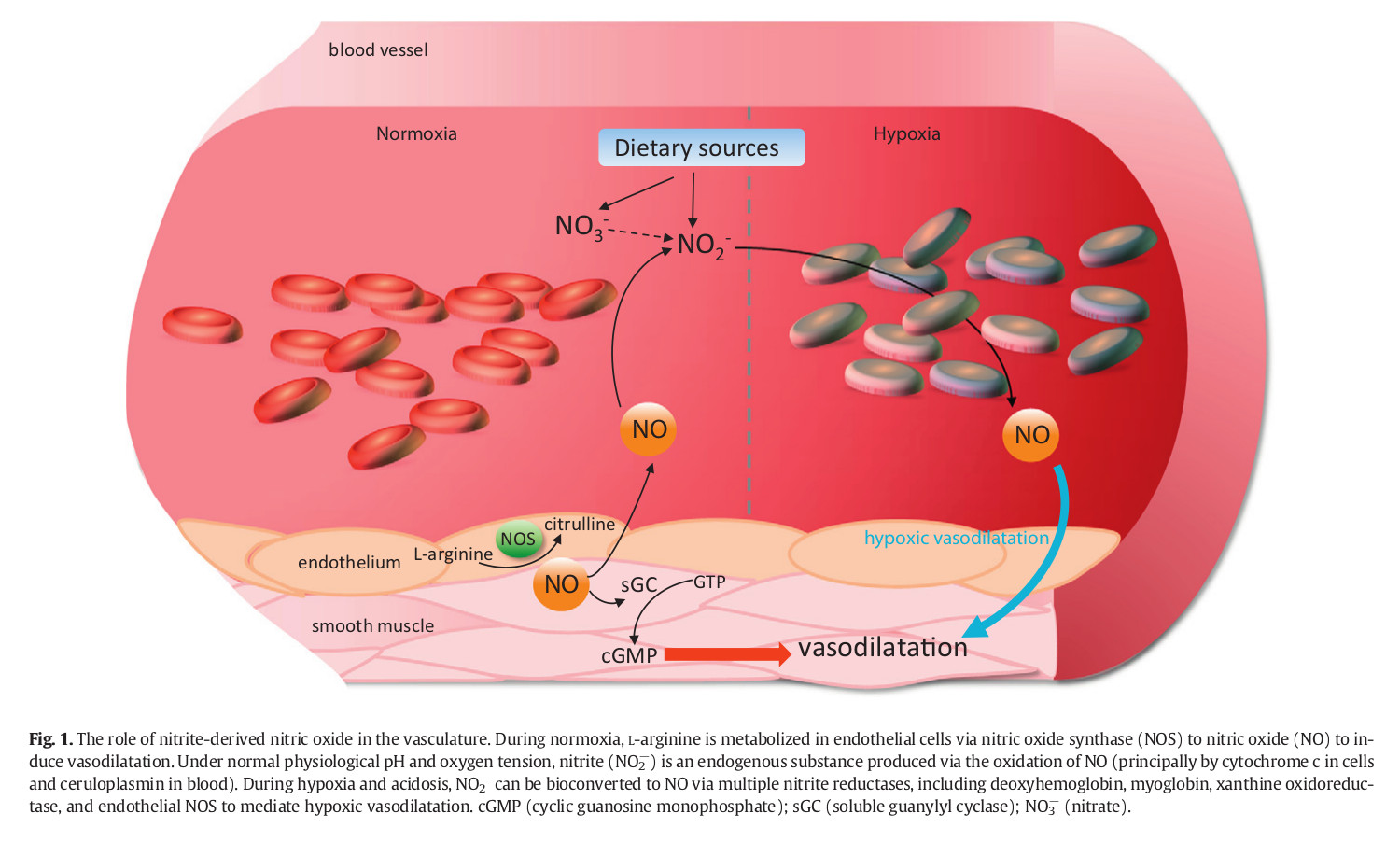
Sodium nitrite, NaNO2, is a catalyst that converts the hemoglobin in blood into methemoglobin (MetHB), a molecule with a much higher affinity with oxygen. This conversion occurs when the ferrous ions in the regular hemoglobin are converted into ferric ones. Since its affinity is so high, methemoglobin does not let the oxygen flow into other tissues that need it thus depriving them of oxygen��even while you��re breathing. Death, then, occurs due to hemolytic anemia or anemic hypoxia, not hypoxic hypoxia. The main reason for peacefulness of sodium nitrite method is that nitrate and nitrite reduce to nitric oxide, a vasodilator. Vasodilators relax hence dilate the smooth muscle in veins. Dilating veins will cause fall in blood pressure and loss of consciousness. (Bailey, Feelisch, Horowitz, Frenneaux & Madhani, 2014) illustrated the nitrite-derived NO signalling[1|2|3].
Sodium nitrite poisoning symptoms include nausea, vomiting, vertigo, headaches, and tachycardia. All of these symptoms will not emerge in everyone. These symptoms will provide low level discomfort, and you will suffer no discomfort through the process. As for the physical symptoms, the color of blood, skin, fingertips, nail beds, and lips will change. The blood will take a bluish chocolate brown color, and the tips of fingers, toes, and nose will turn slightly blue from cyanosis (PubChem). In April 2019, a kindergarten teacher in China poisoned 23 children by lacing their breakfast with sodium nitrite. The only noticeable change in appearance of kindergarten students were their lips that had turned blue[1|2|3|4]. Additionally, in September 2019, four members of an Indian family committed suicide using sodium nitrite; similarly, little change to bluish[1|2|3|4|5|6] was visible in the color of their skin, their fingertips, and blood[1|2|3|4]. Also, (Warren and Blackwood, 2019) published a case report of a 25-year-old woman who had used benzocaine. The percentage of methemoglobin in her blood was 44%. The patient appeared cyanotic and had dark arterial and venous blood[1|2|3]. She was treated with intravenous methylene blue and had considerable improvement in her breathing and reduction in skin discoloration. Putting on a proper makeup[1|2|3|4] to go out in style can conceal any changes in your appearance.Sodium Nitrite - Suicide Wiki
https://suicide.wiki/w/Sodium_Nitrite��
SODIUM NITRITE AS ANTIDOTE FOR CYANIDE/ACRYLONITRITE POISONING
Indication: Cyanide/acrylonitrite
Mode of Action: Nitrites facilitate conversion of hemoglobin to methemoglobin. Methemoglobin has higher binding affinity to cyanide which further facilitates its excretion.
Dosage: 10mL of 3% sodium nitrite solution through IV for 5-20 minutes followed by sodium thiosulphateDrugs & Their Antidotes: A Nurse's Ultimate Guide - NurseBuff
https://www.nursebuff.com/common-drugs-and-their-antidotes/��
.png)
.png)