烟酸、冠心病和长寿
Niacin,
Coronary Disease and Longevity
by Abram Hoffer,
M.D., Ph.D.
翻译:蓝山
Hoffer A. Niacin, Coronary Disease and Longevity. J Orthomolecular Medicine 4:211-220, 1989.
很多科学的发现都带有偶然性,候弗无意中发现烟酸可以帮助愈合他的牙龈出血,由此最终发现烟酸可以降低过高的血胆固醇水平、以及治疗很多相互无关的疾病,包括癌症。。。人的健康和生病都基于自身的体质,而营养素和体质的关系不容置疑。更重的是,烟酸在体内转化为NAD(烟酰胺腺嘌呤二核苷酸),即辅酶。这很好解释了烟酸可以及快速、有效的治疗多种互不相关的疾病的原因-译者
背景
1954年,是没有可能预测或想到,我出血的牙龈会在31年后的某一日,能够帮助与胆固醇和类脂代谢有关的冠心病的人过得更好。哪一年,我的牙齿的咬合不正已经破坏了我的牙龈的快速自我修复能力。因为我咬牙方法不正确,导致牙藏磨损太厉害,我的牙龈开始出血。无论多大数量的维生素C和牙科修复都不能有效止血。最后,我已有这样的念头,不久的将来,我所有的牙齿都要拨掉。
但到此时,我已用烟酸治疗精神分裂症和老年病以及其它一些疾病。因而,我也开始服用这种维生素,每顿饭后1克,每日3次,即每天3克。我这样做的原因是,我要体验这种首次服用烟酸后的潮红(继续服用潮红会逐渐减轻),以方便我可以更有知识地和病人讨论。同时也有一个法律上的问题—大多数医生面对付诉讼的理据是,他们只是做其他医生在相同情况下做的处理。如果我因为烟酸引起的异常不适或副作用而被起诉(我从未被起诉过),我不能使用这条理据,因为只有几个医生曾经使用过这么大剂量的烟酸。我断定,如果不可能的情况真的出现,我因此而被告以治疗失当,我的其中一个理据将会是我自己亲自试验了超过3个月而没有造成严重的不良效果。我必须承认,我没有跟我的律师讨论过此事。因此我的推理既是可行的,也是多疑的。我并无有任何治疗我自己或我的牙龈的意图。
在我开始服用烟酸的二个星期后我的牙龈康复了。一个早上,我在擦牙时,我突然发现无论如何擦拭都不会流血!几天过后,我的牙医证实我的牙龈不再肿胀,而到现在,我仍然保留大部分的牙齿。最后,我推断烟酸已经恢复了我的牙龈组织的自我修复能力。
几个月后,萨斯喀彻温大学医学院解剖系的Rudl Altschul教授找我。他以前教神经组织学,我曾经是他的学生之一。Rudl Altschul教授发现了在兔产生动脉粥样硬化的方法。他给这此兔喂食他夫人用蛋黄做的烤蛋糕。这些喂烤蛋糕的兔很快产生高胆固醇血症,紧接着在冠状动脉出现粥样硬化性损害(Altschul and Herman, 1954)。Altschul亦发现用紫外线灯照射这些高胆固醇血症的兔会降低它们的胆固醇水平。他要在人体进行相同的照射以扩大他的研究。但在萨斯卡通没有一个内科医生允许他在他们的病人身上进行这样的试验。习惯在南方晒太阳的人可能会觉得奇怪,为什么这种“危险的”治疗遇到如此消极的反应。Altschul教授因而找我。作为萨斯喀彻温大学卫生系精神治疗研究的主任,我可以接触我们二间精神病医院的几千名病人。我提出,在萨斯喀彻温Weyburn医院的负责人Humphry Osmond也同意的前提下,我就同意他的要求。这种治疗是无害的,不会造成任何损失而同时会帮助我们的临床员工开阔研究的视野。但在开始前,我要求Altschul教授会见我们的临床医生并向他们介绍将要进行的实验。
几周后,他坐火车到Regina,我开车送他去Weyburn会见Osmond和他的全体职员。在往返途中,我讨论我们的研究。他有趣地向我介绍了他发现的动脉粥样硬化问题的看法。他认为动脉粥样硬化是血管内膜的一种疾病。他猜测内膜失去了快速自我修复的能力。听到此,我马上联想到我的牙龈出血以及我自己的修复假设。然后我告诉他我最近的经历。我问他是否愿意试验烟酸是否同样对内膜有相同的效果,因为烟酸对我的牙龈可能有抗粥样硬化的作用。这引起了Altschul教授的兴趣,并且说如果能得到一些烟酸,他同意考虑这个想法。我马上送给他一磅纯正、结晶的烟酸。这些烟酸是我早些时候收到的一个供应商(默克公司,现在的默沙东)的慷慨赠与。
约三个月后的一个晚上,我接到Altschul教授打来的电话。他一开始就呼叫,“烟酸 有效!烟酸有效!” 然后他告诉我,他给他的高血脂水平的兔喂食烟酸,几天之内,它们的胆固醇水平回复到正常水平。他已发现了第一个降低胆固醇的物质。制药公司正在花费百万的金钱去发现这样的一种复合物。
但烟酸在人身上也有效吗?第二天,我向Regina 总医院的病理学家J. Stephen博士请教。我是他的生物化学顾问。我简要地介绍了已做的实验,并要求他帮助做一些人体的临床实验。我向他保证烟酸是安全的。我们只需给病人几克的烟酸。他马上就同意了。他说,他将要求他的技术人员从大量病人中抽取血液作胆固醇检测,然后给病人烟酸。之后再抽取血液进行另一次检测。我建议我们先征求病人的私人医生的意见,但Stephen博士笑着说,他们不知道医院进行的情况,如果要联系每一人私人医生,会使这个研究变得不可能。几个星期后,结果开始出来:烟酸也降低人体的胆固醇水平。初始值越高,下降幅度越大。
我们发表了我们的研究结果(Altschul, Hoffer and Stephen, 1955)。这份报告引发了最终证明烟酸可延长寿命的相关研究。因为他的重要性,这份报告在这里再一次出版。注意,这不是一个双盲实验。然而,病人不知道他们正在服用的药物或他们要服用的原因。因为道德委员会、知情权以及其它的因素,这种类型的即席研究以后都不再可能了。30年前,只有医生的正直可以保护病人免受有害的实验。
在我们试验烟酸对胆固醇水平的影响时,前苏联的科学家也在检测维生素对血脂的影响,但他们使用很少量的烟酸,因而发现无明显的下降(Simonson and Keyes ,1961)。
这个烟酸可以降低胆固醇的发现不久被Parsons, Achor, Berge, McKenzie 和Barker (1956) and Parsons (1961, 1961a, 1962)证实。而Mayo诊所按自己的方式把烟酸作为一个降胆固醇的药物。自此以后,烟酸被证实是一种令胆固醇正常的因子,即是说,它升高高密度脂蛋白胆固醇,降低密度脂蛋白胆固醇和极低密度脂蛋白胆固醇以及甘油三酯水平。Grundy, Mok, Zechs and Berman (1981)发现它可降低胆固醇达22%而甘油三酯达52%,并说,就我们所知,没有其它任何物质具有同时降低胆固醇和甘油三酯的功效。”
冠心病研究
关注高胆固醇水平的唯一原因是它和冠心病发病率的升高有关。膳食中胆固醇水平的高低和冠心病的相关性并不是完全对应,虽然整体饮食是一个主要的因素。基本上正分子医生推荐的饮食将倾向于降低大部分人的胆固醇水平。这种饮食可以描述为一种高纤维素、不含糖而含丰富复杂的多聚糖比如蔬菜和粗粮的饮食。
一旦可以降低胆固醇水平而不需要改变饮食,就可以验证降低胆固醇水平会减少患冠心病的风险的假说。当时在华盛顿的国家健康研究院的E. Boyle博士很快对烟酸产生兴趣。他开始跟踪一系列的病人对每天3克烟酸的反应。在一份由Bill W (1968)起草准备发给酒精匿名会的医生的报告中他公布了他的实验结果。在这份报告里,Boyle博士指出,他让160名冠心病病人连续服用烟酸10年,只有6人在其中死亡(而按统计学上的估计,如果接受常规治疗,62人已经死亡)。他强调指出,“从严格的医学角度上讲,我相信若所有病人都服用烟酸,他们会活得更久并更能享受生命。”
最近Canner对国内冠心病药物研究的评估令他的预测得到证实。但E. Boyle博士的数据已经很有说服力了。也许Boyle博士的研究是1966年冠心病药物研究的原因之一。Boyle博士是这个研究的顾问之一。这个研究是要在8341个30~64岁,至少过去3个月曾经发生心肌梗塞(心脏病发作)的男性病人当中,评估5种复合物的长期效果及其安全性。
国家心脏和肺脏医学会支持此项研究。它在全国的26个州的53个诊所进行。目的是要检测几种降脂药的效果,以及确定降低胆固醇对曾患心肌梗塞的病人是否同样有效。测试的药物包括烟酸、二种不同剂量的雌激素、安妥明、右旋甲状腺素以及安慰剂。
试验开始后的18个月,高剂量的雌激素组因为新的非致命性心肌梗塞的出现(对比安慰剂组)而中止。甲状腺素组同样因为引起有特发生室性心动过速的病人心肌梗塞而中止。36个月后,余下的右旋甲状腺素成员同样因为心肌梗塞发生率增加而中止。56个月后,低剂量的雌激素组中止。低剂量雌激素对增加的肺栓塞和血栓性静脉炎无明显的改善作用。最后,只有烟酸、安妥明和安慰剂组直到研究的结束。
Canner's的研究(1985)
巴尔的摩马利兰医学研究院的首席统计员Paul L. Canner博士,分析了冠心病药物研究小组的数据。约8000人在1975年研究结束时仍然生存。这个分析在1981年开始,目的是判断二种雌激素以及右旋甲状腺素方案是否产生任何长期的效果。高剂量雌激素因为增加非致命性心肌梗塞而中止,低剂量雌激素增加癌症死亡率,而右旋甲状腺素增加总体的死亡率,也就是,对比安慰剂、安妥明和烟酸。1975年后,再没有任何人继续服用以上药物。
1985年的跟综调查显示,在所有接受治疗的小组中,中途中止的小组、安慰剂组或安妥明组之间,在死亡率方面没有明显的差异。然而,令调查者惊奇的是,烟酸组的病人生活得更好。低雌激素组、高雌激素组、安妥明组、右旋甲状腺组、安慰剂以及烟酸组的总体死亡率分别是58.4%、56.8%、55.9%、56.9%和50.6%。
烟酸组的死亡率比安慰剂组的少11%(P=0.002)。烟酸减少死亡的益处体现在每个主要的分类或死亡原因:冠心病、其它心血管病、癌症和其它。分析烟酸组和安慰剂的生命图表曲线,烟酸组病人比安慰剂组病人多活二年。平均14年的跟综调查,烟酸组病人比安慰剂病人少死亡70人。胆固醇水平高于240 毫克/100毫升的病人比哪些更低水平的人受益更大。
令人惊奇的是,烟酸的益处持续很长的时期,即使停止服用之后。事实上,跟踪调查越往后,其益处越来越大。如果没有在1975年停止服药,结果很可能会更好。因而,E. Boyle博士的病人,因为坚持服用了10年,并且得到更到位的跟踪服务,取得了少90%的死亡率。作为大规模的冠心病研究,这种对大多数到位的跟踪服务是不可能的。许多人中途退出的原因是烟酸引起的潮红,而这些人如果得到更多的关注,相当多的人可能会坚持进行实验。Boyle博士和我讨论时,提到这是这个冠心病研究的不足之处。我会做出这样的结论,作为期10年的跟踪调查,烟酸对类似病人的适当使用会减少死亡率约11%和90%之间。随着死亡率的下降,烟酸作为安全的天然物质的程度上升,从而减少死亡率,增加寿命,尤其是高胆固醇水平很高的病人。
国家健康研究院(1985)公布了1984年12月10~12日举行仪的关于降低胆固醇以预防心脏病的研讨会的一致结论。随后发表一份声明,“降低胆固醇以预防心脏病,”第5卷,第7。这个声明指出,心脏病每年导致550,000美国人死亡以及540万美国人患有心脏病。每年为此开支达600亿美元。主要的危险因素包括吸烟、高血压和高血清胆固醇。国家健康研究院建议治疗的第一措施应该是饮食,而他们的饮食建议可通过正分子饮食而得到满足。但饮食尚不足够时,应该配合药物。胆酸盐螯合剂和烟酸应被首选。而主要的商业化药物—Clofibrate,而不建议使用,因为“它对大部分的高血清胆固醇水平而甘油三脂水平正常的病人无效。 另外,世界卫生组织对此种药物的试验发现总体死亡率太高。”
因为烟酸只有在大剂量(每次1克,每天3次)使用时才有效,国家健康研究院最终推广大剂量维生素疗法。国家健康研究院要求他们的会议声明要被“张贴、复印和分发到每个相关的人士”。因为每个医生都有高胆固醇症的病人,他们都应该感兴趣。事实上,如果他们对此不感兴趣,一部分医生将会受到得不到烟酸治疗高胆固醇的病人的愤怒的妻子的起诉。
烟酸结合其它降低胆固醇的药物
家族性高胆固醇血症是一种血浆胆固醇水平很高的遗传性疾病。Illingworth, Phillipson, Rapp 和Connor(1981)叙述了用Colestipol治疗一系列的13名病人,先进行每天10克分二次服用,之后每天15克,分三次服用。病人的胆固醇水平从345MG/ML~524MG/ML,而甘油三脂水平从70MG/ML~232MG/ML。当些药物不能降低胆固醇至270MG/ML,病人改用烟酸治疗。开始剂量为250MG/次,每天三次。持续2~4星期后增加剂量。直到每天的剂量达3~8克。为了减低潮红,每次让病人加服120~180MG的阿斯匹林持续4~6星期。在这种剂量下,没有发现病人的肝功能检查结果异常。这种药物配合恢复了病人的胆固醇和血脂水平。他们得出结论,“大多数杂合性家族性高胆固醇血症的病人,用一种胆酸螯合剂配合烟酸治疗,可令胆固醇和血脂水平回复正常或接近正常。这类病人常常会过早出现动脉粥样硬化,而这种方案的长期应用为这类病人提供预防、或甚至逆转过早出现的动脉粥样硬化的可能性。”
大约在同时,Kane, Malloy, Tun, Phillips, Freedmand, Williams, Rowe 和 Havel (1981)报告了在一系列共50个病人取得了类似的结果。他们亦研究了Colestipol 和Clofibrate的配合效果。肝功能异常只在烟酸剂量快速提高的情况下才产生。第一个月,他们每天口服2.5克烟酸,第二个月每天5克而从第三个月开始每天7.5克。少数病例的血糖水平轻度升高(从115升高到120MG),而6个病人的尿酸水平超过8MG。没有任何病人出现痛风症。所有检查结果均正常。他们得出结论,“Colestipol和烟酸的配合降低LDL(低密度胆固醇脂)以及缩小腱黄瘤的显著效果提示,这种配合是现时改变动脉粥样硬化症的最可行的治疗方案。” Colestipol 和Clofibrate的配合效果比不上前者。这是历史上第一次有可能延长这类家族性高胆固醇血症病人的寿命。
幸运地,烟酸不会把胆固醇下降到危险的过低水平。Cheraskin 和 Ringsdorf (1982)评估了低胆固醇水平和癌症发生率升高以及总体死亡率上升的关系的一些证据。Ueshima, Lida 在 Komachi (1979)发现胆固醇水平在150~200MG/ML和脑血管疾病的负相关关联(r = .83)。胆固醇水平低于160MG/ML时,死亡率上升。
Hoffer和Callbeck (1957)报告,烟酸的降低血浆胆固醇的作用和自主神经系统的活动有关。我们提到一个此前由Altschul 和Hoffer进行的研究,在这个研究中,我们发现在志愿者(医学院学生)中,烟酸降低胆固醇的作用和最初的胆固醇水平,以及体重呈线性关系。衰退等式是Y = 0.95X - 0.39Z – 90,这里,Y是胆固醇下降的数量,以毫克计算,X是最初的胆固醇值而Z是体重,单位是磅。多相关系数是0.83。当Y=0时,烟酸对胆固醇水平无任何影响。当Y是负数是,意味着胆固醇水平可被烟酸提高。这可能是最佳胆固醇水平的一种提示。对一个200磅的病人当X=176MG时,Y=0,, 而对一个150磅的病人,当X=156MG,Y=0。这个跟Cheraskin、 Ringsdorf 和其他人推荐的最佳值非常接近,即,180~200MG。
Hoffer和Callbeck发现,烟酸亦降低精神分裂症病人的胆固醇水平,但精神分裂症病人的反应以一种不同的等式Y = 0.28X -0.43Z + 53表示。这个在以下的图表显示,在这里,预期的胆固醇下降数量用二种不同的等式算出(参看第220页的图表)即,在超出正常值的高水平,烟酸降低更大的胆固醇水平,而在低胆固醇水平,烟酸并不升高胆固醇水平。再一次,烟酸升高正常人的胆固醇水平,从150MG到176MG,降低胆固醇水平从200MG降到178MG,而从250MG降到181MG。
烟酸如何产生作用?
只是烟酸,而不是烟酰胺降低胆固醇水平,即使二种形式的维生素B3都有抗脚气病的作用,而且在治疗精神分裂症和关节炎以及其它疾病中其效果几乎相同。烟酸和烟酰胺不同,因为它引起潮红,很多人会逐渐适应,而烟酰胺在99%的服用者中没有血管扩张的作用。因为一些尚不清楚的原因,大约有1%的服用者会产生潮红。他们必定是在体内能把烟酰胺快速转化为烟酸。当中必定有一些线索。一般认为,烟酸通过一个复杂的机制导致组织胺的释放,干扰前列腺素代谢,或者和血色素机制有关,或者涉及胆碱系统(Rohte, Thormahlen and Ochlich (1977))从而产生潮红。
组织胺明显相关。典型的烟酸潮红和注射组织胺产生的潮红完全相同。如果不用抗组胺药和镇静药预防,这种潮红现象逐渐减轻。对烟酸的适应可以用贮存部位如肥大细胞中组织胺的减少很容易地解释。当组织胺释放后再检查这些细胞时,这些细胞中原来贮存组织胺和类肝素的小泡已经变成空囊。如果服用烟酸的间隔足够密,将没有时间让这些贮存组织胺的小泡再补充组织胺。因而,可分泌的组织胺更少。在完全适应烟酸后,如果停药几天,潮红周期将会再现。这种组织胺的减少对减轻快速组织胺释放的效应有一定程度的好处。Ed Boyle医生发现,经烟酸处理后的豚鼠不会受到过敏性休克的伤害。因为潮红是相对暂时的,它不可能是涉及降低胆固醇的机理,因为烟酸降低胆固醇的作用是伴随整个服药过程的。前列腺素看来关。因而,阿斯匹林(Kunin ,1976)和吲哚美辛(,Kaijser, Eklund, Olsson and Carlson 1979)可以减潮红的程度( Estep, Gray and Rappolt, 1977)。
1983年,我提出因为它释放组织胺和粘多糖,烟酸可以降低胆固醇。烟酰胺没有此种作用(Hoffer, 1983)。Mahadoo, Jaques 和 Wright (1981)早些时候暗示在脂质吸收和再分布过程中的一个组织胺-粘多糖组织胺酶系统。Boyle (1962)发现烟酸增加嗜碱性白细胞数。这些细胞贮存肝素以及组织胺。他认为由烟酸产生的改善作用比它对胆固醇的作用更大。他说:“可能” “因为组织胺的释放,同时亦是最终血管内红细胞凝集的明显减少所至”。
可能,烟酸的益处不是因为它降低胆固醇,而是由于一个更基本的机制。升高的胆固醇水平和动脉粥样硬化两者是否是一个更基本的代谢失调的终极结果仍然未被证实?如果它完全是由于降低胆固醇的效果,为什么Clofibrate没有相同的益处?将来某日破解出烟酸的其它特性或许可以导致这个基本代谢失调的揭开。烟酸具有快速的抗凝作用。瘀血是在红细胞凝聚在一起时发生。瘀血不能穿过毛细血管,因为毛细血管只能容纳一个红细胞通过。瘀血瘀塞血管导致组织不能获得它们的红细胞分配,从而导致缺氧。烟酸可以改变红细胞膜的表面特性,令它们不能互相粘连。组织因而可能得到需要的血液。烟酸的作用十分迅速。烟酸加速康复,正如它康复我的牙龈一样。或者它对血管损伤的内皮有类似的作用。
在过去的几年,有人提出肾上腺素通过它的肾上腺色素衍生物在冠心病中发挥作用。如果得到证实,它将为烟酸对心脏病的益处提供另一个解释。Beamish 和他的同事 (1981, 1981a, 1981b)在一系列的报告中展示,心肌组织会摄取肾上腺素,而肾上腺素会转化为肾上腺色素。而正是肾上腺色素导致心室纤维颤动以及心肌损伤。他们更加发现,Anturan防止由肾上腺色素引起的心室纤维颤动,并且认为,这个被Anturan可减少心脏病的死亡率的临床发现所支持。
在严重的紧张情况下,如休克或注射肾上腺素后,血液中发现大量的肾上腺素并被心肌组织吸收。严重的紧张因而是是否有动脉粥样硬化的一个诊断因子,但亦可能是动脉粥样硬化的心脏不能应付紧张。心室纤维颤动会增加心肌的耗氧量,而一个冠状动脉已受损的心脏不能满足这种需要。
在体内,烟酸保护组织免受肾上腺色素的毒性作用的影响。它可以逆转癫痫者静脉内注射肾上腺色素后诱发的心电图改变(Szatmari, Hoffer and Schneider ,1955),亦可以逆转心理改变(Hoffer and Schneider ,1955)。在突触,NAD在维持去甲肾上腺素和肾上腺素在还原态中是必不可少的。这些儿茶酚氨失去一个电子后形成氧化型氨。在NAD存在的情况下,这个复合物还原为它的最初的儿茶酚氨。如果缺乏NAD,氧化态的肾上腺素(或去甲肾上腺素)会失去另一个电子,形成肾上腺色素(或去甲肾上腺色素)。这个改变是不可逆转的。肾上腺色素是一个突触阻滞剂,如同LSD。因而,烟酸,通过维持NAD的水平减少肾上腺色素的形成。这很可能也在心肌内发生同样的作用,而如果确实如此,它将保护心肌组织免受肾上腺色素的毒性损害,以及预防心室纤维颤动和组织坏死。没有已知的其它降低胆固醇物质具有这种保护作用。烟酸因而具有一个优势:(1)降低胆固醇和,(2) 降低心室纤维颤动的发生率以及减轻组织损伤。
烟酸作为急性冠心病的一种治疗
Altschul (1964)翻查了在心脏梗塞发生后的第一时间使用烟酸治疗的临床资料。Goldsborough (1960)以这种方式同时使用烟酸和烟酰胺。给冠状动脉血栓症的病人皮下注射50毫克的烟酸,并舌下含服100毫克。在潮红的出现的同时,疼痛和休克缓解。当潮红减退时,疼痛再发生则给予另一次注射。但如果疼痛不严重,给予烟酸口服。然后,他给予每天三次,每次100毫克口服。如果潮红过于严重,他改用烟酰胺。
从1946年到1960年,他治疗了60个病人,其中24个是急性心肌梗塞,其余是心绞痛患者。在这24个心肌梗塞病人中,6个死亡。其中4个心绞痛病人同时有间歇性跛行,亦得到缓解。2个有肺栓塞者亦有改善。
应在冠状动脉搭桥手术前后给予烟酸。Inkeless 和 Eisenberg (1981)翻查了冠状动脉搭桥术和血脂水平有关的证据。目前对冠状动脉搭桥术是否增加生存率仍没有取得一致意见。大多数情况下,生命的质量得到提高,而75%的病人的心绞痛得到部分或全部的缓解。我相信搭桥手术的一个尚未解决的主要问题是如何控制粥样硬化的进程。Inkeles 和 Eisenberg指出,在动脉内的自生血管移植比动脉更容易产生粥样硬化。在55个生存了13到26个月的病人体内共99处的隐静脉移植的解剖研究中,粥样硬化出现在78%有高血脂症的病人的搭桥动脉内。主动脉-冠状动脉搭桥加速原来的血管的闭塞过程。
如果病人经常被给予适当的饮食,以及如果在形成任何冠心病前的很早就开始服用烟酸,如果不是全部,大部分的搭桥手术可以避免。如果每个需要做搭桥手术的病人都给予适当的饮食,以及在搭桥手术后给予足够的烟酸,粥样硬化的进程将会显著减慢。那么,搭桥术将显著延长有用的寿命。病人希望看到顶级心脏手术和顶级内科医生运用饮食和降低胆固醇的技术的结合。
小结
烟酸延长曾经有过心肌梗塞的病人的寿命并减少死亡率。1985年4月24日出版的The Medical Tribune杂志,以醒目的标题“一个意外的长寿关联元素:烟酸。”( A Surprise Link to Longevity: It's Nicotinic Acid) 适当地表达了调查者对结果的反应,如果他们认真对待Ed Boyle的发现,他们就不会觉得惊奇,并且取得了更好的调查结果。
备注:1982年,Keats出版了我对维生素B3(烟酸)的调查结果。那份调查只是重点介绍烟酸许多益处的其中一个方面。应当二份同时阅读,因为二者是并列的报告。
经已查明,烟酸的衍生物降低血脂水平的能力和烟酸同样出色。如果烟酸的血管扩张(潮红)作用被消除,将会更显优势。烟酸衍生物的主要问题是成本。Inositol hexanicotinate是一种酯化的肌醇和烟酸。在体内,它缓慢水解释放出这二种重要的营养素。这种酯在降低胆固醇和甘油三脂水平方面更有效(Abou El-Enein, Hafez, Salem and Abdel 1983)。我使用过这种复合物, Linodil,加拿大有这种药,但美国没有(在写本报告时)。对过去的三十年哪些不能耐受潮红的病人,这是一种十分温和、有效、并且几乎所有使用者都可以耐受的药物。
不仅对心血管疾病,烟酸对其它疾病在减少死亡率以及延长寿命方面都有效。它的作用原理是保护细胞和组织不受毒性分子或自由基的损害。
其中一个令信兴奋的发现是烟酸将保护你不受癌症的侵袭。今年早些时候在Fort Worth的得克萨斯骨病医学学院举办的会议,是第八届讨论烟酸与癌症的会议(Titus,1987).。第一届会议于1984年在瑞士举行。
在体内,烟酸转化为烟酰胺腺嘌呤二核苷酸(NAD)。NAD是许多反应中的一种辅酶。另一种酶,多聚(ADP-核糖)合成酶,需要NAD催化二磷酸腺苷-核糖的形成。香烟、除草剂等会裂解DNA股,从而激活多聚(ADP-核糖)合成酶。当长链NDA受到损害,多聚(ADP-核糖)合成酶通过展开受损的蛋白质而帮助修复DNA。多聚(ADP-核糖)合成酶也增加DNA连接酶的活性。这种酶剪开受损的DNA股,并且增加细胞在接触致癌物质后的自我修复的能力。
Jacobson 和Jacobson (Hostetler ,1978)相信烟酸(更具体地,NAD)抑制癌变的过程。他们发现,一组给予足够烟酸的人类细胞,然后让其接触致癌物质,产生癌症的比率仅是没有给予烟酸的同一组细胞的10份之一。癌细胞中NAD含量低于正常细胞。
在国家冠心病药物研究中发现烟酸减少癌症死亡率是毫不奇怪的。我治疗的第一个癌症病例我给予每天烟酸3克和每天维生素C3克(Hoffer ,1970)。
烟酰胺亦增加NAD的合成。每天3克给青少年糖尿病患者获得很高的显效率(Vague, Vialettes, Lassman-Vague, and Vallo ,1987)。他们得出总论,“我们的结果,以及动物实验结果表明,对I型糖尿病,烟酰胺减缓B细胞的破坏,增加B细胞的再生,因而延长了完全缓解时间。”(参看 Yamada, Nonaka, Hanafusa, Miyazaki, Toyoshima and Tarui ,1982)。烟酰胺保护肾组织(Wahlberg, Carlson, Wasserman and Ljungqvist ,1985)。烟酸保护大鼠对抗链脲佐菌素诱生糖尿病的效应。临床上,烟酸曾经成功治疗严重肾小球性肾炎病人。我的其中一个病人曾准备做透淅。她的肾科医生曾告诉她,如果她拒绝透淅治疗,她就会死去。她开始了每天3克烟酸的治疗。25年后,她现在仍然健康。
烟酸和烟酰胺对多种疾病有保护作用。我仅指出其中的一种或二种作用去减少霍乱的水液流失(Rabbani, Butler, Bardhan and Islam ,1983)。它抑制和逆转由霍乱毒素或大肠埃希菌外毒素(E. coli enterotoxin)导致的肠道分泌。它减少与胰腺肿瘤引起的泄泻。
现在清楚表明,维生素B3是一种强力的良性的物质,涉及身体内的多种反应,并且在大剂量时,对很多种显明无关联的疾病产生治疗和保护作用。所有这些疾病是否是由于饮食或毒素在体内的积聚造成的维生素B3缺乏状态的次要的和主要的表现呢?
很有可能,任何一个增加维生素B3摄入量的人,即使只是每天100毫克,而已经患有各种疾病的人,服用更大剂量的烟酸,将会导致死亡率的显著减少以及寿命的增加。
Background
In 1954, it was impossible to predict or even to think that my bleeding gums would one day, 31 years later, lead to additional useful life to people with coronary disease related to cholesterol and lipid metabolism. That year, malocclusion of my teeth had broken down the ability of my gum tissue to repair itself quickly enough. Because my bite was not correct there was too much wear and tear on tooth sockets and my gums began to bleed. No amount of Vitamin C and no amount of dental repair helped. Eventually I reconciled myself to the idea I would soon have all my teeth extracted.
But at this time I had been treating schizophrenics and seniles and a few other diseases with niacin, and I began also to take this vitamin, 1 gram after each meal, i.e. three grams per day. I did so because I wanted to experience the flush which comes when one first takes niacin and its gradual waning with continuing use so I could discuss this reaction more know-ledgeably with my patients. There was also a legal issue — most doctors’ defence against malpractise suits is that they were doing what any other similar physician would do it like circumstances. If I were sued (I have never been sued) because of unusual discomfort or because of adverse effects from niacin, I would not be able to use that defence since only a handful of physicians had ever used these large quantities of niacin. I had concluded that if the unlikely did occur and I was charged with malpractise, one of my defences would be that I had tried it myself for at least three months without suffering any serious consequences. I must admit I had not discussed this with any litigation lawyer. My reasons were therefore both practical and paranoid. I had no intention of treating myself or my bleeding gums.
Two weeks after I had started taking niacin my gums were normal. I was brushing my teeth one morning and suddenly awakened in surprise — there was no bleeding whatever! A few days later my dentist confirmed my gums were no longer swollen, and I still have most of my teeth. Eventually I reasoned that the niacin had restored the ability of my gum tissue to repair itself faster than I could damage it by chewing with my crooked teeth.
A few months later I was approached by Prof. Rudl Altschul, Chairman, Department of Anatomy, College of Medicine, University of Saskatchewan. He had taught neurohistology and I had been one of his students. Prof. Altschul had discovered how to produce arteriosclerosis in rabbits. He fed them a cake baked by his wife, Anna, which was rich in egg yolks. Rabbits fed cooked egg yolk promptly developed hypercholesterolemia and later arteriosclerotic lesions on their coronary vessels, Altschul and Herman (1954). Altschul had also discovered that irradiating these hypercholesterolemic rabbits with ultraviolet light decreased their cholesterol levels. He wanted to extend this research by irradiating human subjects, but not one internist in Saskatoon would allow him access to their patients. People who bake in the southern sunshine may wonder why this “dangerous” treatment received such a negative response. Prof. Altschul thus approached me, as Director of Psychiatric Research, Department of Health, Saskatchewan, I had access to several thousand patients in our two mental hospitals. I agreed to this provided that Dr. Humphry Osmond, Superintendent of the Saskatchewan Hospital at Weyburn also agreed. This treatment was innocuous, would not cost us anything and would help us create more of an investigative attitude among our clinical staff. But before we started I requested that Prof. Altschul meet with our clinical staff and present his ideas to them.
A few weeks later he came to Regina by train and I drove him to Weyburn in my car to meet Dr. Osmond and his staff. On the way down and back we discussed our work. He gave me an interesting review of how he saw the problem of arteriosclerosis, which he considered to be a disease of the intima, the inner lining of the vessels. He hypothesized that the intima had lost its ability to repair itself quickly enough. As soon as I heard this I thought of my bleeding gums and of my own repair hypothesis. I then told him of my recent experience. I asked him if he would be willing to test niacin which if it had the same effect on the intima as it had had on my bleeding gums might have antiarteriosclerotic power. Prof. Altschul was intrigued and agreed to look at the idea if he could get some niacin. I promptly sent him one pound of pure, crystalline niacin from a supply I had received earlier, courtesy of Merck and Company, now Merck, Sharp and Dohme. One evening about three months later I received a call from Prof. Altschul who began to shout, “It works! It works!” Then he told me he had given niacin to his hypolipidemic rabbits and within a few days their cholesterol levels were back to normal. He had discovered the first hypocholesterolemic substance. Drug companies were spending millions to find such a compound.
But did it also work in humans? The next day I approached Dr. J. Stephen, Pathologist, General Hospital, Regina. I was a biochemical consultant to him. I outlined what had been done and wanted his help in some human experiments. I assured him niacin was safe and we would only need to give a few grams to patients. He promptly agreed. He said he would order his technicians to draw blood for cholesterol assay from a large variety of patients, would then given them niacin and would follow this with another cholesterol assay. I suggested we discuss this with the patients’ physicians but Dr. Stephen laughed and said they did not know what went on in hospital and that to contact each one would probably make the study impossible. A few weeks later the data poured in: niacin also lowered cholesterol levels in people. The greater the initial or baseline level, the greater the decrease. We published our results (Altschul, Hoffer and Stephen, 1955). This report initiated the studies which eventually proved niacin increases longevity. Because of its importance, this paper is reproduced here. Note, it was not double blind. However, patients did not know what they were getting or why they were getting it. This type of impromptu research is forever impossible with ethics committees, informed consent and so on. Thirty years ago only the integrity of physicians protected patients against experimental harm.
At the same time we were examining the effect of niacin on cholesterol levels, Russian scientists were also measuring the effect of vitamins on blood lipids but they used very little niacin and found no significant decreases, Simonson and Keyes (1961).
The finding that niacin lowered cholesterol was soon confirmed by Parsons, Achor, Berge, McKenzie and Barker (1956) and Parsons (1961, 1961a, 1962) at the Mayo Clinic which launched niacin on its way as a hypercholesterolemic substance. Since then it has been found to be a normalizing agent, i.e. it elevates high density lipoprotein cholesterol, decreases low density and very low density lipoprotein cholesterol and lowers triglycerides. Grundy, Mok, Zechs and Berman (1981) found it lowered cholesterol by 22 percent and triglycerides by 52 percent and wrote, “To our knowledge, no other single agent has such potential for lowering both cholesterol and triglycerides.”
The Coronary Study
The only reason for being concerned about elevated cholesterol levels is that this is associated with increased risk of developing coronary disease. The association between cholesterol levels in the diet and coronary disease is not nearly as high even though the total diet is a main factor. The kind of diet generally recommended by Orthomolecular physicians will tend to keep cholesterol levels down in most people. This diet can be described as a high fiber, sugar-free diet which is rich in complex polysaccharides such as vegetables and whole grains.
Once it became possible to lower cholesterol levels even with no alteration in diet, it became possible to test the hypothesis that lowering cholesterol levels would decrease the risk of developing coronary disease. Dr. E. Boyle, then working with the National Institute of Health, Washington, D.C., quickly became interested in niacin. He began to follow a series of patients using 3 grams of niacin per day. He reported his conclusions in a document prepared for physicians in Alcoholics Anonymous by Bill W (1968). In this report Boyle reported that he had kept 160 coronary patients on niacin for ten years. Only six died against a statistical expectation 62 would have died with conventional care. He stated, “… from the strictly medical viewpoint I believe all patients taking niacin would survive longer and enjoy life much more.”
His prediction came true when the National Coronary Drug Study was evaluated by Canner recently. But E. Boyle’s data spoke for itself. Continuous use of niacin will decrease mortality and prolong life. Perhaps Boyle’s study was one of the reasons the Coronary Drug Project was started in 1966. Dr. Boyle was an advisor to this study which was designed to assess the long term efficacy and safety of five compounds in 8341 men, ages 30 to 64, who had suffered a myocardial infarction at least three months before entering the study.
The National Heart and Lung Institute supported this study. It was conducted at fifty-three clinical centres in twenty-six American states and was designed to mea-sure the efficacy of several lipid lowering drugs and to determine whether lowering cholesterol levels in patients with previous myocardial infarcts would be beneficial. Niacin, two dosage strengths of estrogens, Clofibrate, dextrothyroxine and placebo were tested.
Eighteen months after the study began, the higher dose estrogen group in the study was discontinued because of an excess of new non-fatal myocardial infarctions compared to placebo. The thyroxine group was stopped for the same reason for patients with frequent ectopic ventricular beats. After thirty-six months dextrothy-roxin was discontinued for the rest of this group, again because myocardial infarcts were increased. After fifty-six months the low dose estrogen group study was stopped. There had been no significant benefit to compensate for the increased incidence of pulmonary embolism and thrombophlebitis and increased mortality from cancer. Eventually only niacin, Clofibrate and placebo groups were continued until the study was completed.
Canner’s Study (1985)
Dr. Paul L. Canner, Chief Statistician, Maryland Medical Research Institute, Baltimore, examined the data for the Coro-nary Drug Project Research Group. About 8000 men were still alive at the end of the treatment trial in 1975. This new study was begun in 1981 to determine if the two estrogen regimens and the dextrothyroxine regimen had caused any long term effects. High dose estrogen had been discontinued because it increased non-fatal myocardial infarctions, low dose estrogen increased cancer deaths and dextrothyroxine increased total mortality, i.e. compared to placebo, Clofibrate and niacin. None of the subjects continued to take the drugs after 1975.
The 1985 follow-up study showed no significant differences in mortality between those treatment groups which had been discontinued and placebo or Clofibrate. However, to the investigator’s surprise, the niacin group fared much better. The cumulative percentage of deaths for all causes was 58.4%, 56.8%, 55.9%, 56.9% and 50.6% for low dose estrogens, high dose estrogens, Clofibrate, dextrothyroxine, placebo and niacin, respectively. The mor-tality in the niacin group was 11 percent lower than in the placebo group (P = 0.002). The mortality benefit from niacin was present in each major category or cause of death: coronary, other cardiovascular, cancer and others. Analysis of life table curves comparing niacin against placebo showed the niacin patients lived two years longer. With an average follow-up of fourteen years, there were 70 fewer deaths in the niacin group than would have been expected from the mortality in the placebo group. Patients with cholesterol levels higher than 240 mg per 100 mL benefitted more than those with lower levels.
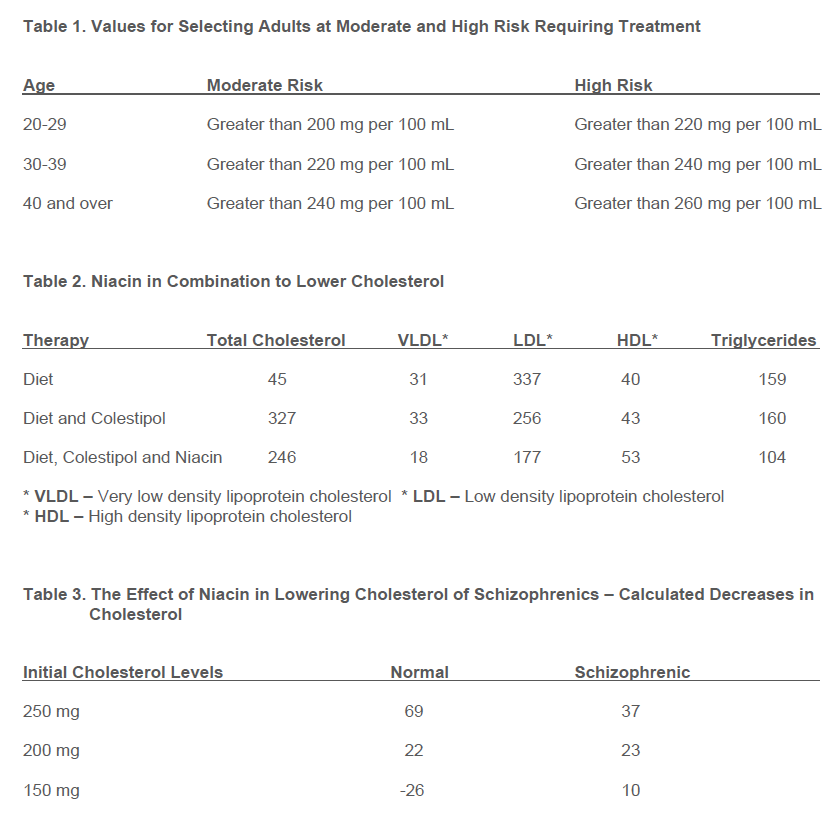
What is surprising is that the niacin benefit carried on for such a long period even after no more was being taken. In fact the benefit increased with the number of years followed up. It is highly probable the results would have been much better if patients had not stopped taking niacin in 1975. Thus, E. Boyle’s patients who remained on for ten years and received individual attention had a 90 percent decrease in mortality. With the huge coronary study this type of individual attention for the majority of patients was not possible. Many dropped out because of the niacin flush, of these many could have been persuaded to remain in the study if they had been given more individual attention. This is very hard to do in a large scale clinical study of this type. Dr. Boyle, in discussions with me, referred to this as one of the defects in the Coronary Drug Study. I would conclude that the proper use of niacin for similar patients should decrease mortality somewhere between 11 and 90 percent after a ten year follow-up, with the reduction in mortality increasing as the safe natural substance which will decrease mortality and increase longevity especially in patients with elevated cholesterol levels. The National Institute of Health (1985) released the conclusions reached by a consensus development conference on lowering blood cholesterol to prevent heart disease held December 10 – 12, 1984. This was followed by an NIH conference statement, “Lowering Blood Cholesterol to Prevent Heart Disease”, Volume 5, No. 7. This statement reports that heart disease kills 550,000 Americans each year and 5.4 million are ill. Total costs of heart disease are $60 billion per year. Main risk factors include cigarette smoking, high blood pressure and high blood cholesterol. The relationship of age and cholesterol levels to risk is shown below. (See Table 1 page 220.)
NIH recommends that the first step in treatment should be dietary and their recommendations are met by the Ortho-molecular diet. But when diet alone is not adequate, drugs should be used. Bile-acid sequestrants and niacin are favoured while the main commercial drug, Clofibrate, is not recommended “because it is not effective in most individuals with a high blood cholesterol level but normal triglyceride level. Moreover, an excess of overall mortality was reported in the World Health Organization trial of this drug.” Since niacin is effective only in megavitamin doses, 1 gram three times per day, NIH is at last promoting megavitamin therapy. The National Institute of Health asked that their conference statement be “posted, duplicated and distributed to interested staff”. Since every doctor has patients with high blood cholesterol levels, they should all be interested. In fact, if they are not, some of them will be facing litigation from angry wives whose husbands have not been treated with niacin for their elevated cholesterol levels.
Niacin Combined With Other Drugs Which Lower Cholesterol
Familial hypercholesterolemia is an inherited disease where plasma cholesterol levels are very high. Illingworth, Phillip-son, Rapp and Connor (1981) described a series of 13 patients treated with Colestipol 10 grams twice daily and later 15 grams twice daily. Their cholesterol levels ranged from 345 to 524 and triglycerides from 70 to 232. When this drug plus diet did not decease cholesterol levels below 270 mg/100 mL they were given niacin, starting with 250 mg three times daily and increasing it every two to four weeks until a final dose of 3 to 8 grams per day was reached. To reduce the flush patients took aspirin (120 to 180 mg) with each dose for four to six weeks. With this dose of niacin they found no abnormal liver function test results. This combination of drugs normalized blood cholesterol and lipid levels. (See Table 2, page 220.)
They concluded, “In most patients with heterozygous familial hypercholesterolemia, combined drug therapy with a file acid sequestrant and nicotinic acid results in a normal or near normal lipid profile. Long term use of such a regimen affords the potential for preventing, or even reversing, the premature development of athero-sclerosis that occurs so frequently in this group of patients.”
At about the same time Kane, Malloy, Tun, Phillips, Freedmand, Williams, Rowe and Havel (1981) reported similar results on a larger series of 50 patients. They also studied the combined effect of Colestipol and Clofibrate. Abnormalities of liver function only occurred when the dose of niacin increased rapidly. The first month they took 2.5 grams per day, the second month 5.0 grams per day and 7.5 grams per day the third month and thereafter. In a few, blood sugar went up a little (from 115 to 120 mg), and uric acid levels exceeded 8 mg percent in six. None developed gout. All other tests were normal. They concluded, “The remarkable ability of the combination of Colestipol and niacin to lower circulating levels of LDL and to decrease the size of tendon xanthomas suggests that this combination is the most likely available egimen to alter the course of atherosclerosis.” The combination of Colestipol and Clofibrate was not as effective. For the first time it is possible to extend the life span of patients with familial hypercholesterolemia.
Fortunately, niacin does not decrease cholesterol to dangerously low levels. Cheraskin and Ringsdorf (1982) reviewed some of the evidence which links low cholesterol levels to an increased incidence of cancer and greater mortality in general. Ueshima, Lida and Komachi (1979) found a negative correlation between cholesterol levels between 150 and 200 and cerebral vascular disorders (r = – .83). Mortality increased for levels under 160 mg.
Hoffer and Callbeck (1957) reported that the hypercholesterolemic action of niacin was related to the activity of the autonomic nervous system. We referred to a previous study by Altschul and Hoffer where we found on normal volunteers (medical students) that there was a linear relationship between the effect of niacin in lowering cholesterol, the initial cholesterol levels and body weight. The regression equation was Y = 0.95X – 0.39Z – 90 where Y is the decrease in cholesterol level in milligrams, X is the initial cholesterol value and Z the body weight in pounds. The multiple correlation coefficient is 0.83. When Y = O niacin has no effect on cholesterol levels. When Y is negative it means the cholesterol levels were elevated by niacin. This might then be a good indication of the optimum cholesterol levels. For a 200 pound patient Y = O when X is 176 mg, and for a 150 pound subject Y = O when X is 156 mg. This is remarkably close to the optimum values recommended by Cheraskin and Ringsdorf and others, i.e. 180 to 200 milligrams. Hoffer and Callbeck found that niacin also lowered cholesterol levels of schizophrenic patients, but the schizophrenic response was represented by a different equation Y = 0.28X -0.43Z + 53. This is shown in the following table where expected decreases in cholesterol are calculated from two equations. (See Table 3 page 220.) i.e. at higher levels niacin decreases choles-terol levels more in normal subjects while at lower levels niacin did not increase the level of cholesterol. Again niacin elevated levels in normal subjects from 150 to 176, decreased it from 200 to 178 and from 250 to 181 mg.
How Does Niacin Work?
Niacin, but not niacinamide, lowers cholesterol levels even though both forms of Vitamin B-3 are anti pellagra and are almost equally effective in treating schizophrenia and arthritis and a number of other diseases. Niacin also differs from niacinamide because it causes a flush to which people adapt readily while niacinamide has no vasodilation activity in 99 percent of people who take it. For reasons unknown, about 1 in 100 persons who take niacinamide do flush. They must be able to convert niacinamide to niacin in their bodies at a very rapid pace. There must be a clue here somewhere. It is believed that niacin causes a flush by a complicated mechanism which releases histamine, interferes in prostaglandin metabolism, may be related to serotonin mechanism and may involve the cholinergic system, Rohte, Thormahlen and Ochlich (1977). Histamine is clearly involved. The typical niacin flush is identical with the flush produced by an injection of histamine. It is dampened down if not prevented entirely by anti-histamines and by tranquilizers. The adaptation to niacin is readily explained by the reduction in histamine in the storage sites such as the mast cells. When these are examined after a dose of histamine, these cells contain empty vesicles which contained the histamine and also heparinoids. If the next dose is spaced closely enough there will have been no time for the storage sites to be refilled and therefore less histamine will be available to be released. After there is complete adaptation to niacin a rest of several days will start the flushing cycle again. This decrease in histamine has some advantage in reducing the effects of rapidly released histamine. Dr. Ed Boyle found that guinea pigs treated with niacin were not harmed by anaphylactic shock. Because the flush is relatively transient it can not be involved in the lowering of cholesterol which remains in effect as long as medication is continued. Prostaglandins appear to be involved. Thus, aspirin, Kunin (1976), and indomethacin, Kaijser, Eklund, Olsson and Carlson (1979) reduce the intensity of the flush, Estep, Gray and Rappolt(1977).
In 1983 I suggested that niacin lowered cholesterol because it releases histamine and glycosaminoglycans. Niacinamide does not do so, Hoffer (1983). Mahadoo, Jaques and Wright (1981) had earlier implicated a histamine-glycosaminogly-can histaminase system in lipid absorption and redistribution. Boyle (1962) found that niacin increased basophil leukocyte count. These cells store heparin as well as histamine. He suggested that the improvement caused by niacin is much greater than can be explained by its effect on cholesterol. “Possibly,” he wrote, “it is due to release of histamine and also to the eventual marked diminution in the intra-vascular sludging of blood cells.”
It is possible the beneficial effect of niacin is not due to the cholesterol effect but is due to a more basic mechanism. Are elevated cholesterol levels and arteriosclerosis both the end result of a more basic metabolic disturbance still not identified? If it were entirely an effect arising from lowered cholesterol levels, why did Clofibrate not have the same beneficial effect? An enumeration of some other properties of niacin may one day lead to this basic metabolic fault.
Niacin has a rapid anti sludging effect. Sludged blood is present when the red blood cells clump together. They are not able to traverse the capillaries as well, as they must pass through in single file. This means that tissues will not receive their quota of red blood cells and will suffer anoxemia. Niacin changes the properties of the red cell surface membrane so that they do not stick to each other. Tissues are then able to get the blood they need. Niacin acts very quickly.
Niacin increases healing, as it did with my gums. Perhaps it has a similar effect on the damaged intima of blood vessels. Within the past few years adrenalin via its aminochrome derivatives has been im-plicated in coronary disease. If this becomes well established it provides another explanation for niacin’s beneficial effect on heart disease. Beamish and his coworkers (1981, 1981a, 1981b) in a series of reports showed that myocardial tissue takes up adrenalin which is converted into adrenochrome, that it is the adrenochrome which causes fibrillation and heart muscle damage. They further found that Anturan protects against fibrillation induced by adrenochrome and suggest this is supported by the clinical findings that Anturan decreases mortality from heart disease. Under severe stress as in shock or after injection of adrenalin, a large amount of adrenalin is found in the blood and absorbed by heart tissue. Severe stress is thus a factor whether or not arteriosclerosis is present, but it is likely an arteriosclerotic heart can not cope with stress as well. Fibrillation would increase demand for oxygen which could not be met by a heart whose coronary vessels are compromised.
Niacin protects tissues against the toxic effect of adrenochrome, in vivo. It reverses the EEG changes induced by intravenous adrenochrome given to epileptics, Szatmari, Hoffer and Schneider (1955), and also reverse the psychological changes, Hoffer and Osmond (1967). In synapses NAD* is essential for maintaining nora-drenalin and adrenalin in a reduced state. These catecholamines lose one electron to form oxidized amine. In the presence of NAD this compound is reduced back to its original catecholamine. If there is a deficiency of NAD the oxidized adrenalin (or noradrenalin) loses another electron to form adrenochrome (or noradrenochrome). This change is irreversible. The adrenochrome is a synaptic blocking agent as is LSD. Thus niacin which maintains NAD levels decreases the formation of adrenochrome. It is likely this also takes place in the heart and if it does it would protect heart muscles from the toxic effect of adrenochrome and from fibrillation and tissue necrosis. None of the other substances known to lower cholesterol levels are known to have this protective effect. Niacin thus has an advantage: (1) in lowering cholesterol and, (2) in decreasing frequency of fibrillation and tissue damage.
Niacin as a Treatment for Acute Coronary Disease
Altschul (1964) reviewed the uses of niacin clinically where it is used as soon as possible after an acute event. Goldsbor-ough (1960) used both niacin and niacinamide in this way. Patients with a coronary thrombosis were given niacin 50 mg by injection subcutaneously and 100 mg sub-lingually. As the flush developed the pain and shock subsided. If pain recurred when the flush faded another injection was given, but if pain was not severe another oral dose was used. Then he used 100 mg three times daily. If the flush was excessive he used niacinamide. Between 1946 and 1960 he treated 60 patients, 24 with acute infarction and the rest with angina. From the 24 patients, six died. Four of the angina patients also had intermitten claudication which was relieved. Two had pulmonary embolism and also responded.
Niacin should be used before and after every coronary bypass surgery. Inkeless and Eisenberg (1981) reviewed the evidence related to coronary artery bypass surgery and lipid levels, there is still no consensus that this surgery increases survival. In most cases the quality of life is enhanced and 75 percent get partial or complete relief of angina. I believe a major problem not resolved by cardiovascular surgery is how to halt the arteriosclerotic process. Inkeles and Eisenberg report that autogenous vein grafts implanted in the arterial circuit are more susceptible than arteries to arteriosclerosis. In an anatomic study of 99 saphenous vein grafts from 55 patients who survived 13 to 26 months, arteriosclerosis was found in 78 percent of hyper-lipidemic patients. Aortic coronary bypass grafting accelerates the occlusive process in native vessels.
If patients were routinely placed on the proper diet and if necessary niacin long before they developed any coronary problems, most if not all the coronary bypass operations could be avoided. If every patient requiring this operation were placed upon the diet and niacin following surgery, the progress of arteriosclerosis would be markedly decreased. Then surgeons would be able to show a marked increase in useful longevity. One would hope to have the combined skills of a top cardiac surgeon and a top internist using diet and hypo-cholesterolemic compounds.
Conclusion
Niacin increases longevity and decreases mortality in patients who have suffered one myocardial infarction. The Medical Tribune, April 24, 2985, properly expressed the reaction of the investigators by heading their report, “A Surprise Link to Longevity: It’s Nicotinic Acid.” Had they taken Ed Boyle’s finding seriously they would not have been surprised and would have gotten even better results.
Note: In 1982 Keats published my review of Vitamin B-3 (Niacin). This present review concentrates in greater detail on only one aspect of niacin’s many beneficial properties. The two should be read together as they are companion reports.
Derivatives of niacin have been examined for their ability to alter lipid levels as well as niacin. It would be advantageous if the niacin vasodilation (flush) were eliminated or removed. The main disadvantage of the niacin derivatives will be cost. Inositol hexanicotinate is an ester of inositol and niacin. In the body it is slowly hydrolzyed releasing both of these important nutrients. The ester is more effective than niacin in lowering cholesterol and triglyceride levels, Abou El-Enein, Hafez, Salem and Abdel (1983). I have used this compound, Linodil, available in Canada but not the U.S.A., for thirty years for patients who can not or will not tolerate the flush. It is very gentle, effective, and can be tolerated by almost every person who uses it.
Niacin is effective in decreasing the death rate and in expanding longevity for other conditions, not only cardiovascular diseases. It acts by protecting cells and tissues from damage by toxic molecules or free radicals.
One of the most exciting findings is that niacin will protect against cancer. A con-ference at Texas College of Osteopathic Medicine at Fort Worth early this year, was the eighth conference to discuss niacin and cancer, Titus (1987). The first was held in Switzerland in 1984.
In the body niacin is converted to nicotinamide adenine dinucleotide (NAD). NAD is a coenzyme to many reactions. Another enzyme, poly (Adenosine adenine phosphate ribose) polymerase, uses NAD to catalyze the formation of ADP-ribose. The poly (ADP-ribose) polymerase is activated by strands of DNA broken by smoke, herbicides, etc. When the long chains of DNA are damaged, poly (ADP-ribose) helps repair it by unwinding the damaged protein. Poly (ADP-ribose) also increases the activity of DNA ligase. This enzyme cuts off the damaged strands of DNA and increases the ability of the cell to repair itself after exposure to carcinogens.
Jacobson and Jacobson [Hostetler (1978)] believe niacin (more specifically, NAD) prevents processes which lead to cancer. They found that one group of human cells given enough niacin and then exposed to carcinogens developed cancer at a rate only one-tenth of the rate in the same cells not given niacin. Cancer cells are low in NAD. It is not surprising that niacin also decreased the death rate from cancer in the National Coronary Drug Study. The first cancer case I treated was given niacin 3 grams per day and ascorbic acid 3 grams per day, Hoffer (1970).
Niacinamide also increases the production of NAD. Three grams per day given to juvenile diabetics produced remissions in a large proportion of these young patients, Vague, Vialettes, Lassman-Vague, and Vallo(1987). They concluded, “Our results and those from animal experiments indicate that, in Type I diabetes, nicotinamide slows down the destruction of B cells and enhances their regeneration, thus extending remission time.” See also Yamada, Nonaka, Hanafusa, Miyazaki, Toyoshima and Tarui (1982). Kidney tissue is protected by niacinamide, Wahlberg, Carlson, Wasserman and Ljungqvist (1985). It protected rats against the diabetogenic effect of Streptozotocin. Clinically niacin has been used to successfully treat patients with severe glomerulonephritis. One of my patients was being readied for dialysis. Her nephrologist had advised her she would die if she refused. She started on niacin 3 grams per day. She is still well twenty-five years later.
Niacin and niacinamide are protective in a large number of diseases. I will refer to one or more its ability to reduce fluid loss in cholera, Rabbani, Butler, Bardhan and Islam (1983). It inhibits and reverses intestinal secretion caused by cholera toxin and E. coli enterotoxin. It reduces diarrhea associated with pancreatic tumors in man.
It is clear Vitamin B-3 is a very powerful, benign substance which is involved in numerous reactions in the body, and which in larger doses is therapeutic and preventative for a large number of apparently unrelated diseases. Are all these conditions really expressions of minor and major Vitamin B-3 deficiency states due to diet, or to accumulation of toxins in the body?
It is highly likely that any human population which increased the intake of Vitamin B-3 in everyone, by even 100 mg per day and to much higher levels in people already suffering from a number of pathological conditions, will find a substantial decrease in mortality and an increase in longevity.
SOURCE: https://www.isom.ca/article/niacin-coronary-disease-longevity/
参考书目 REFERENCES
Abou EI-Enein AM,
Hafez YS, Salem H and Abdel,
M: The role of
nicotinic acid and inositol hexanicotinate as anticholesterolemic and antilipemic agents. Nutrition
Reports International, 281:899-911, 1983.
Hoffer A: The psychophysiology of cancer. J. Asthma Research, 8:61-76, 1970.
Hostetler, D: Jacobsons put broad strokes in the niacin/cancer picture. The D.O., Vol. 28, August 1987, pp. 103-104.
Rabbani GH, Butler T, Bardhan PK and Islam A: Reduction of fluid-loss in cholera by nicotinic acid. The Lancet, December 24CE31, 1983, pp. 1439-1441.
Titus K: Scientists link niacin and cancer prevention. The D.O., Vol. 28, August 1987, pp. 93-97.
Vague PH, Vialtettes B, Lassmanvague V and Vallo JJ: Nicotinamide may extend remission phase in insulin dependent diabetes. The Lancet, 1:619-620, 1987.
Wahlberg G, Carlson LA, Wasserman J and Ljungqvist A: Protective effect of nicotinamide against nephropathy in diabetic rats. Diabetes Research, 2:307-312, 1985.
Yamada K, Nonaka K, Hanafusa T, Miyazaki A, Toyoshima H and Tarui S: Preventive and therapeutic effects of large-dose nicotinamide injections on diabetes associated with insulitis. Diabetes, 31: 749753, 1982.
免责声明: 本网站全部内容翻译自国外专业网站,所有版属于本站及原作人,未经同意不得转载或出版。同时,网页上的观点仅是原作人的立场,不可作为诊断和治疗疾病的依据。